





Abstract
Bronchoscopic bronchoalveolar lavage (BAL) may be followed by a systemic inflammatory response. Previous reports have suggested pneumonia as a predisposing condition and systemic cytokines as possible mediators.
To test this hypothesis, systemic levels of interleukin (IL)-1β, IL-6 and tumour necrosis factor-alpha (TNF-α) were studied before and at 12 h and 24 h after bronchoscopically guided BAL in 30 mechanically ventilated patients (median age 67 (range 54–76) yrs, simplified acute physiology score II (SAPS II) 33 (12–56)), 20 of whom had pneumonia and 10 of whom were control patients without pneumonia. Arterial oxygen partial pressure to inspired oxygen fraction ratio (Pa,O2/FI,O2), body temperature, mean arterial pressure, and cardiac frequency were recorded. The majority of patients (28/30, 93%) received antibiotic treatment prior to the procedure.
Pa,O2/FI,O2 ratio was lower at 12 h compared to baseline in patients with pneumonia (baseline median 192 (range 65–256); 12 h 160 (66–190) mmHg, p<0.001) and ventilated controls (baseline 293 (205–473); 12 h 226 (153–330) mm Hg p=0.011), but returned to baseline levels at 24 h (pneumonia: 194 (92–312), p=0.991; controls: 309 (173–487) mmHg, p=0.785). No changes in other clinical variables were observed. Systemic TNF-α levels before BAL (pneumonia: 35 (10–88); controls: 17 (0–33) pg·mL−1) did not increase at 12 h (pneumonia: 35 (0–64); p=0.735; controls: 16 (0–21) pg·mL−1, p=0.123 comparison to baseline) or 24 h (pneumonia: 31 (0–36), p=0.464; controls: 19 (0–43) pg·mL−1, p=0.358). No changes of IL-1β (baseline: pneumonia 0 (0–13); controls 1 (0–32) pg·mL−1) or IL-6 (baseline: pneumonia, 226 (9–4300); controls, 53 (0–346) pg·mL−1) were detected.
No deterioration of clinical variables and no increase in systemic cytokine release has been observed after bronchoalveolar lavage, in critically ill patients. The potential cytokine increase is probably too small, in relation to the pre-existing inflammatory response, to yield clinical significance in this population otherwise antibiotic therapy may have been protective.
This work was supported by: Fondo de investigación Sanitaria (FIS) Grant #: 98/1096, 1997, Suport dels Grups de Recerca (SGR) Grant #: 00086, IDIBAPS, Comissió Interdepartmental de Recerca i Innovació Tecnológica (CIRIT, 1999), the European Respiratory Society (ERS), and the Bochumer Arbeitskreis für Peumologie und Allergologie (BAPA).
Fibreoptic procedures, and particularly bronchoalveolar lavage (BAL), are important diagnostic tools, and tolerance is generally good. Side effects such as serious arrhythmia, bleeding, pneumonia, or pneumothorax are rare 1 and acute haemodynamic effects are small even in critically ill intubated patients 2. However, in some cases, BAL may be followed by myalgia, headache or even fever 3. A systematic follow-up after bronchoscopically guided BAL suggested that this systemic inflammatory response, or sepsis-like syndrome, is caused by a proinflammatory cytokine release 4. This study in noncritically ill patients, however, excluded patients with pneumonia, and did not assess the bacterial burden of the lungs. Translocation of bacterial products 5 or even entire micro-organisms 6 from the lungs to the bloodstream, however, may play a crucial role for the pyrogenic response after BAL, particularly in the presence of mechanical ventilation.
Systemic cytokine levels have therefore been studied after bronchoscopically guided BAL in mechanically ventilated patients, with and without pneumonia.
Materials and methods
This trial was conducted in an 850-bed tertiary care hospital between January 1 1995 and December 31 1997. All patients on ventilatory support for more than 48 h in one respiratory intensive care unit (RICU) were eligible for the study. Patients were included consecutively if they fulfilled clinical criteria of pneumonia: presence of new infiltrates on the chest radiograph and two of the following criteria: fever ≥38.3°C, purulent secretions, leukocytosis (≥12,000·mm−3) or leukopenia (≤4,000·mm−3). Pneumonia was classified as community-acquired (occuring <72 h into stay) or nosocomial (≥72 h). The ventilated control group without pneumonia included patients who met the following criteria: 1) mechanical ventilatory support for more than 48 h; 2) absence of any infectious process; or 3) absence of any of the criteria of the pneumonia group. Bronchoscopy was indicated for other reasons (e.g. tube malposition, minor haemoptysis or visual inspection of the tracheobronchial tree) in patients without pneumonia.
Exclusion criteria were: 1) unstable clinical condition (e.g. cardiac arrhythmia, acute ischemic heart disease, need for vasoactive drugs); 2) known increased intracranial pressure; 3) small diameter endotracheal tube (<7 mm); 4) acute respiratory distress syndrome (ARDS); 5) cerebral injury; or 6) coagulation's disorders. The study was approved by Ethical Committee of our Centre and in each case informed consent was obtained from the next of kin.
Protocol
The following demographic, clinical, and laboratory data were recorded from all patients: age; gender; underlying disease; cause of RICU admission; duration of mechanical ventilation before the study; use of corticosteroids (any i.v. administration during 24 h prior to sampling); prior antibiotic use (administered i.v. for more than 24 h); blood analyses necessary for calculations of the simplified acute physiology score (SAPS II) 7. Antipyretic medication (e.g. nonsteroid anti-inflammatory drugs) was not used 24 h prior to the study and was also withheld during the 24 h follow-up period.
Arterial oxygenation expressed as arterial partial pressure of oxygen/inspired fraction of oxygen (Pa,O2/FI,O2), arterial blood pressure, cardiac frequency (fC) and axillary body temperature were sequentially recorded and for the purpose of this study were documented before and at 12 h and 24 h after BAL. An increase in body temperature of ≥1°C within the 24 h follow-up was defined as significant.
Blood sampling
Arterial blood samples were collected anaerobically, through an indwelling polyethylene catheter (Seldicath, Plastimed; Saint-Leu-La-Fôret, France) inserted into the radial artery, before, 12 h and 24 h after BAL, for blood gas and cytokine analyses. These time points were selected because in previous observations, serum tumour necrosis factor-alpha (TNF-α) levels after a fibreoptic procedure were detectable as early as 4 h after the procedure, peaked at 24 h, and returned to undetectable levels by 48 h 8. Samples for blood gases were immersed in ice and processed within 5 min in a blood gas analyser (ABL77 Radiometer, Copenhagen, Denmark). Cytokine samples were collected in sterile tubes without additive and after clotting, were centrifuged at 3.5×g for 10 min. Serum was aspirated and stored at −70°C until processing. Venous blood samples drawn before and 12 h and 24 h after BAL, were cultured for bacterial and fungal pathogens according to standard methods 9.
Bronchoalveolar lavage (BAL)
Patients were sedated before the fiberoptically guided BAL (Pentax FB18, Asahi Optical Ltd., Japan). No local anaesthetics were administered and suction was carefully avoided until the bronchoscope had been wedged in the designated position. A special endotracheal adapter was used in order to continue mechanical ventilation. Patients were ventilated with volume control during bronchoscopy and ventilator settings were readjusted to pre-BAL values thereafter. During bronchoscopy FI,O2 was set to 100% and reduced according to clinical conditions after 1 h. Up to five aliquots of 30 mL physiologic saline were instilled (range 90–150 mL) and the first aspirated portion was discarded. BAL fluid was subjected to microbiological analyses and only pathogens known to cause respiratory infections (potentially pathogenic micro-organisms, PPMs) are reported here.
Cytokine assays
The following cytokines were determined: TNF-α, interleukin-1β (IL-1β) and interleukin-6 (IL-6). Solid phase enzyme-linked immunosorbent assay (ELISA) was employed, based on the quantitative immunometric sandwich enzyme immunoassay technique on a microtitre plate (EASIA: Enzyme Amplified Sensitivity Immunoassay, Medgenix Diagnostics SA, Fleurus, Belgium). This ELISA method used a murine monoclonal antibody specific for the particular cytokine to be analysed, coated onto the microtitre plate to create the solid phase. Serum specimens were pipetted into the wells in duplicate. After the cytokine was bound to the immobilised antibody, a second monoclonal antibody was added to the wells and allowed to bind to a different epitope on the same cytokine. Horseradish peroxidase enzyme was conjugated to the monoclonal antibody. After an incubation period, a sandwich was formed. The enzyme substrate chromagen tetramethylbenzidine was then added and colour developed in proportion to the amount of the particular cytokine bound to the plate. Colour development was stopped with H2SO4, and colourimetric determination was done by means of a polychromic reader (EASIA Reader, Medgenix Diagnostics SA, Fleurus, Belgium). Concentrations of cytokines from samples were determined by comparing the optical densities of the samples to the standard curves. Results are expressed as pg·mL−1 of serum. The sensitivity of the technique allows the detection of levels as low as 3 pg·mL−1 for TNF-α and 2 pg·mL−1 for IL-1β and IL-6, respectively. The following values are regarded as upper limits for cytokine concentrations in normal controls in our laboratory: IL-6 5 pg·mL−1; TNF-α 20 pg·mL−1; and IL-1β 15 pg·mL−1.
Statistical analysis
Results are expressed as median and range because of the nonparametric distribution of the data. The Mann-Whitney U-test was employed for the comparison of quantitative variables between two groups. Changes over time were assessed by Wilcoxon test for paired differences. Proportions were compared by Chi-squared test or Fisher's exact test where appropriate. The level of significance was set to p≤0.05 for all analyses (all two-tailed).
Results
A total of 30 patients were included in the study, 20 (67%) with pneumonia according to the predefined criteria and 10 control patients without pneumonia (33%) (table 1⇓). Pneumonia was nosocomial in 12/20 patients (60%) and community acquired in 8/20 patients (40%). All 20 patients with pneumonia and 8 without pneumonia had received antibiotic drugs prior to BAL. Antibiotics were indicated in control patients for extrapulmonary infections or perioperative infection prophylaxis. Underlying diseases in the pneumonia group included cardiac disease (n=4), chronic obstructive pulmonary disease (COPD, n=5), stroke (n=2), miscellaneous (n=6), and none (n=3). In the control group underlying diseases included: COPD (n=5), miscellaneous (n=3), and none (n=2). Corticosteroid medication had been given to 16/30 (53%) patients prior to the sampling procedure, mainly for bronchial dilatation, without significant differences between patients with pneumonia and controls (table 1⇓). Within the pneumonia group, methylprednisolone had been given for a median 7.5 (1–18) days in a median cumulative dose of 550 (160–1605) mg. The median duration of therapy was 5 (3–8) days in the control group (p=0.859) and the median cumulative dose of 360 (160–705) mg (p=0.440). The mortality observed during RICU stay was 43% (13/30 patients), with a slightly higher mortality among patients with pneumonia (10/20, 50% versus 3/10, 30% p=0.297).
Clinical data of patients investigated
Microbiological data were available in 18/20 (90%) patients with pneumonia and all controls. A total of 7/18 (39%) specimens were sterile. The following PPMs were recovered in the group of patients with pneumonia: Pseudomonas aeruginosa (n=2), Acinetobacter baumanii (n=1), Enterobacter spp. (n=2), Staphylococcus aureus (n=2), Streptococcus pneumoniae (n=2), and Aspergillus fumigatus (n=2). BAL cultures of control patients without pneumonia were sterile or showed no growth for PPMs in 8/10 cases (80%). One BAL showed growth for P. aeruginosa and S. aureus, respectively.
Blood cultures were sterile in all but one patient (29/30, 97%). The pre-BAL blood culture was negative in this particular patient with nosocomial pneumonia, whereas follow-up blood cultures at 12 h and at 24 h showed growth for Streptococcus epidermidis. This micro-organism was also isolated in the BAL fluid of the patient.
Clinical variables
The variation of the Pa,O2/FI,O2 ratio over time for patients with pneumonia and control patients is summarized in figure 1⇓. The Pa,O2/FI,O2 ratio dropped significantly in both groups after the BAL and was significantly lower at 12 h compared to baseline. However, Pa,O2/FI,O2 ratio was indistinguishable from baseline at 24 h (fig. 1⇓). The Pa,O2/FI,O2 ratio was significantly lower in patients with pneumonia compared to controls at any time point (p=0.001, all time points).

Variation of the arterial oxygen partial pressure to inspired oxygen fraction ratio (Pa,O2/FI,O2) over time in patients with (▴: n=20) and without (controls: ⧫; n=10) pneumonia after bronchoalveolar lavage (BAL). Data are presented as means and sds. 1: p=0.017; 2: p=0.001. (p-values are versus pre-BAL using Wilcoxon's test for paired differences).
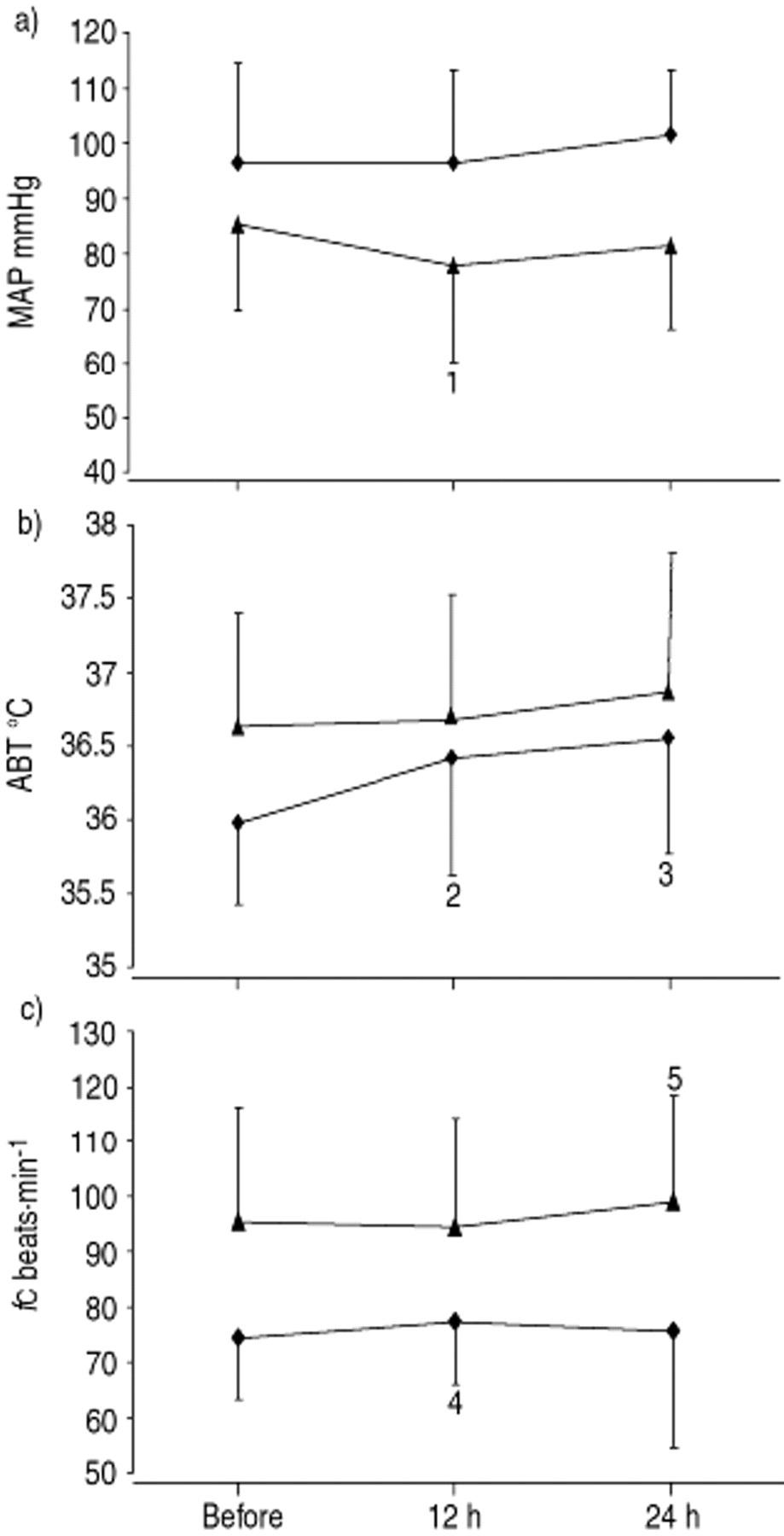
The comparison between patients with pneumonia and controls for mean arterial pressure (MAP), axillary body temperature and fC are illustrated in figure 2⇓. The MAP tended to fall in patients with pneumonia during the first 12 h (p=0.070), but increased again thereafter. No changes were observed in control patients during the follow-up period. A total of 7/30 patients (23%, 3 patients with pneumonia and 4 controls) showed an increase of ≥1°C in body temperature during follow-up. The MAP was different at baseline between patients with pneumonia and controls (p=0.172), but was significantly higher in controls at 12 h (p=0.004) and at 24 h (p=0.001), compared to patients with pneumonia.

{kind=link}
{kind=link}
Comparison of changes in a) mean arterial blood pressure (MAP); b) axillary body temperature (ABT); and c) cardiac frequency (fC) after bronchoalveolar lavage (BAL) in mechanically ventilated patients with (▴; n=20) and without (controls; ⧫; n=10) pneumonia. Data are presented as means and sds. 1: p=0.07; 2: p=0.042; 3: p=0.021; 4: p=0.194; 5: p=0.165. (p-values are versus pre-BAL using Wilcoxon's test for paired differences).
Axillary body temperature increased significantly, only in control patients at 12 h (p=0.042) and 24 h after BAL (p=0.021; fig. 2⇑). Mean values of axillary body temperature were only significantly different between patients with pneumonia and controls before BAL (p=0.01), but not at 12 h (p=0.699) or 24 h (p=0.410; fig. 2⇑).
No significant changes were observed for fC after BAL, neither in patients with pneumonia or the control group (fig. 2⇑). Patients with pneumonia had a higher average fC compared to control patients before BAL (p=0.005) and at 12 h (p=0.009) and 24 h (p=0.009) after BAL.
Systemic cytokine levels
Baseline levels of TNF-α and IL-6 were significantly higher in pneumonia patients compared to controls, reflecting the inflammatory process. However, systemic cytokine expression in serum did not change significantly after BAL in our patients. There was a trend for IL-1β to increase at 24 h and IL-6 tended to fall at this time point (table 2⇓). These changes were caused mainly by the patients in the pneumonia group. The concentration of TNF-α and IL-6 in serum was higher in patients with pneumonia compared to control patients at all time points (table 2⇓), but this was not the case for IL-1β.
Mean systemic cytokine levels before bronchoalveolar lavage (BAL), and 12 h and 24 h thereafter for all the patients and separately for patients with pneumonia and controls
Subanalysis
Data were reanalysed according to the recovery of PPMs in the BAL, because all patients with pneumonia were pre-treated with antibiotics. The results are summarized in table 3⇓. No significant changes over time, or for the comparison of patients with and without pathogens in the lavage, were found.
Comparison of clinical and cytokine data between patients with pneumonia and recovery of a potentially pathogenic micro-organism (PPM) in bronchoalveolar lavage (BAL), and patients with pneumonia and sterile BAL cultures
Pneumonia patients and controls were analysed separately for the comparison of subjects with and without an increase of ≥1°C in body temperature during follow-up, to avoid bias introduced by differences in baseline cytokine levels. Among control patients with an increase in body temperature, only serum IL-6 was significantly higher after 12 h compared to control patients without an increase in body temperature (with increase 81 (51–159) pg·mL−1, no increase 17 (12–55) pg·mL−1, p=0.032). No significant differences for baseline cytokine levels were observed for this comparison. In patients with pneumonia, analysis revealed that those who developed an increase in body temperature showed significantly higher values of TNF-α 24 h after BAL (with increase 61 (59–63) pg·mL−1, no increase 25 (0–49) pg·mL−1 p=0.019).
In another subanalysis, cytokine levels were compared for patients with and without corticosteroid medication also separated for pneumonia patients and controls. In control patients, no differences were found for this comparison in either baseline cytokine levels or during follow-up. Among the patients with pneumonia, baseline serum levels of IL-6 were lower in patients with corticosteroids, compared to those without pneumonia at baseline (with corticosteroids 97 (9–2600) pg·mL−1, no corticosteroids 914 (35–4300) pg·mL−1, p=0.031) and at 12 h follow-up (with corticosteroids 78 (16–2560) pg·mL−1, no corticosteroids 982 (33–3778) pg·mL−1, p=0.041).
Discussion
The findings of this study do not support the hypothesis that pneumonia is a predisposing condition leading to development of a systemic inflammatory response after BAL. This conclusion is based on observations that; 1) bronchoscopically guided BAL in critically ill patients was not associated with clinically significant changes of MAP, body temperature or fC at 12 h or 24 h, regardless of the presence of pneumonia; 2) there was no increase in systemic cytokine release after bronchoscopically guided BAL at 12 h and 24 h in either patients with pneumonia or in controls; 3) a systemic inflammatory response after BAL in patients with pneumonia did not depend on the presence or absence of bacterial pathogens in BAL fluid.
BAL is an important diagnostic tool in critically ill patients. The procedure is generally regarded as safe, and severe side effects rarely occur 3. Most previous studies agree on the fact that BAL induces deterioration of arterial oxygenation 1, 10–12, but these changes are of transient nature. This observation was confirmed in the present study, where all patients, regardless of whether they had pneumonia or not, showed a lower Pa,O2/FI,O2 ratio at 12 h, but returned to or above baseline at 24 h (fig. 1⇑). However, apart from changes in gas exchange, bronchoscopically guided BAL may be followed by fever and other symptoms that have been summarized as sepsis-like effects. The mechanisms that are associated with these sepsis-like symptoms are not known, although they may occur in as many as 30% of the fibreoptically guided procedures 3. Previous reports, however, suggested that the release of pro-inflammatory cytokines may be involved.
Pugin and Suter 13 investigated clinical effects of a fibreoptically guided BAL in critically ill patients with and without pneumonia. They found a significant increase in body temperature and decrease in MAP after the procedure in patients with pneumonia but not in controls. Changes in body temperature correlated significantly with those in MAP, and also with the level of endotoxin in bronchoscopic BAL fluid. These findings suggested that BAL, in critically ill patients with pneumonia, may have caused intravascular translocation of toxins or mediators producing pyrogenic and hypotensive effects. The data from the present study supports this hypothesis only in part, because no general increase in the systemic inflammatory response, as measured by cytokine levels, could be found at 12 h or 24 h. Similarly, no statistically or clinically significant changes in body temperature, MAP or fC could be found after the bronchoscopically guided BAL. It is plausible that differences from the previous study are accounted for by the fact that all but two of our patients had received antibiotic treatment before sampling. Systemic cytokine release, associated with bacterial translocation, may have been blunted by this treatment. On the other hand, one might also argue that the increase in body temperature reported by Pugin and Suter 13 was less likely due to the diagnostic procedure, but due to pneumonia. However, when patients with and without an increase in body temperature ≥1°C during the follow-up period were compared, an increase in IL-6 in control patients after 12 h was seen that was no longer significant after 24 h. It is likely that a transient inflammatory response was described in this subgroup of patients without pneumonia, that may have been associated with the diagnostic procedure. This should be confirmed, though, in a larger cohort, because the number of control patients in the present study was small, and the definition of a temperature increase had to be arbitrary.
A significant systemic cytokine release after BAL has been observed in previous studies involving noncritically ill patients. In a report of a normal healthy volunteer who underwent bronchoscopy and BAL, Standiford et al. 8 showed rising TNF-α levels associated with clinical symptoms after the intervention. Krause et al. 4 systematically compared the systemic inflammatory response after bronchoscopy with and without BAL in 50 patients, with a variety of pulmonary conditions including pulmonary metastasis or bronchial carcinoma. They found an increase of systemic levels of IL-1β and IL-6 at 6 h in all patients, although the increase seemed to be more pronounced in the BAL group. Baseline cytokine levels, however, were low in this noncritically ill population and the mean increase was 27.5 pg·mL−1 for IL-6. Regarding the present study in critically ill patients, an increase of this magnitude was not detectable, and probably not clinically important, because e.g. the IL-6 median level was already more than 30-fold at baseline (108 pg·mL−1) compared to the baseline median (3.71 pg·mL−1) reported in the study by Krause et al. 4 (table 2⇑). In addition, TNF-α levels and particularly IL-6 levels were already well above the normal upper limits for healthy controls at baseline.
This study included one case of possible translocation of S. epidermidis from the pulmonary compartment to the bloodstream after BAL in a 74-yr old female with bilateral nosocomial pneumonia, who had been on mechanical ventilation with zero positive end-expiratory pressure (PEEP) for more than 24 h. Bacteraemia has been described after rigid bronchoscopy, but has never been documented after fibreoptic procedures in humans 4, 14. Animal data suggest that this route of dissemination may have been facilitated by mechanical ventilation 6 or injury to the alveolar epithelium 15. Verbrugge et al. 16 determined the effect of PEEP on the development of bacteraemia with Klebsiella pneumoniae after mechanical ventilation of intratracheally inoculated rats, and concluded that 10 cmH2O PEEP reduced ventilation-induced K. pneumonia bacteraemia. Nevertheless, a causal relationship to the fibreoptic procedure cannot be confidently assumed from the present study, since bacteraemia is a common finding in patients with nosocomial pneumonia, or it may have occurred spontaneously 17. In addition, S. epidermidis is not a common nosocomial pathogen and the assumed translocation from alveolar space to bloodstream may have been unrelated to the underlying inflammatory process. Furthermore, when the systemic inflammatory response was analysed with respect to the presence or absence of potentially pathogenic micro-organisms in the BAL fluid, no significant differences in the systemic inflammatory response after bronchoscopically guided BAL were found.
One might argue that this study simply missed the increase in the systemic inflammatory response, because only two time points were assessed (12 h and 24 h). However, Krause et al. 4 observed differences at 6 h and the well documented case report suggested a peak response at 24 h. However, it cannot be ruled out that short-term changes were missed due to the study design, or changes in the local inflammatory response because patients were not investigated with a follow-up bronchoscopy. A major confounding factor in this study was probably the antibiotic treatment. In fact a trend was even observed towards lower IL-6 levels at 24 h, which could possibly reflect the adequacy of treatment and the decreasing systemic inflammatory response. Nevertheless, it is important not to extrapolate the results to a population without pre-emptive antibiotic therapy. To assist bronchodilatation, a considerable proportion of the patients had received corticosteroids prior to the study, which have been shown to interfere with cytokine levels 18. The comparison between patients with and without corticosteroid treatment was hampered by substantial differences in cytokine levels at baseline between patients with pneumonia and controls, as it has been described previously 18. A multivariate analysis would have been interesting to separate effects of BAL and corticosteroids on cytokine kinetics. However, the present study was too small to allow a reasonable application of this statistical method.
In conclusion, whereas bronchoscopically guided bronchoalveolar lavage seems to be associated with a clinically significant systemic cytokine release in the noncritically ill patient, no general confirmation of this finding in a population of intubated and mechanically ventilated patients could be made. One possible explanation may be that the magnitude of the induced systemic inflammatory response may be insignificant in critically ill patients with high baseline cytokine levels. A transient increase in interleukin-6 levels was observed among patients without pneumonia after 12 h when patients with and without an increase in body temperature were compared, but limitations apply to this subanalysis. Future trials should assess whether antibiotic or corticosteroid pre-treatment has any effect on the systemic inflammatory response after bronchoscopic procedures.
- Received March 23, 2000.
- Accepted September 29, 2000.
- © ERS Journals Ltd
References









