





Abstract
The current authors aimed to examine whether cystic fibrosis (CF) patients in Belgium shared Pseudomonas aeruginosa genotypes and to compare the genotypes of isolates from the same patients during two consecutive years. A Belgian databank of the P. aeruginosa genotypes of all colonised CF patients was created.
Sputum samples from a total of 276 P. aeruginosa colonised patients during 2003, and from a subgroup of 95 patients in 2004, were analysed. Patients were asked about any social contact between each other by questionnaire. All P. aeruginosa isolates exhibiting different colonial morphology on McConkey agar were first genotyped using arbitrarily primed PCR, whereafter single representatives of each randomly amplified polymorphic DNA-type were further genotyped by fluorescent amplified fragment length polymorphism analysis.
In the 213 patients from whom P. aeruginosa could be cultured (resulting in 910 isolates), a total of 163 genotypes were found. The majority (75%) of patients harboured only one genotype. In most of the limited number of clusters, previous contacts between patients could be suspected. In 80% of the patients studied during both years, P. aeruginosa genotype remained unchanged.
In conclusion, most colonised cystic fibrosis patients harbour only one Pseudomonas aeruginosa genotype, despite showing different colonial morphotypes. The number of clusters is limited, and most patients seem to retain the same genotypic strain during both years.
Pseudomonas aeruginosa, widely spread in soils and water, has been the leading pathogen in cystic fibrosis (CF) lung pathology since the 1970s 1–3. The means by which this organism is acquired are not yet fully elucidated. After initial infection, chronic infection and colonisation, as defined by the criteria of Döring et al. 4, cause destruction of lung tissue and reduction of lung function, finally leading to early death. According to the CF Foundation (Bethesda, MD, USA) database of 1996, the median survival age for P. aeruginosa-colonised CF patients was 28 yrs, while the median survival age for noncolonised patients was 39 yrs 5. Kerem et al. 6 demonstrated that patients colonised with P. aeruginosa at the age of 7 yrs had a mean forced expiratory volume in one second 10% lower than that of noncolonised patients.
Currently, some CF centres report the spread of highly transmissible P. aeruginosa strains that are multi-drug resistant and, in some patients, are responsible for primary infection 7–12. Other studies, however, have not found evidence of clonal spread 13–16.
In Belgium, the total number of CF patients registered in the Belgian registry in 2003 was 843 17, of whom 750 were followed at seven CF centres (Sint-Vincentius Hospital/University Hospital Antwerp, HUDERF-Erasme Hospital Brussels, University Hospital of the Free University of Brussels, University Hospital Ghent, University Hospital Leuven, University Hospital Liège, and Hospital of the Catholic University of Louvain-la Neuve) and 280 were considered as colonised by P. aeruginosa, according to the criteria of Döring et al. 4.
This study prospectively set up a Belgian databank of P. aeruginosa genotypes isolated from colonised CF patients to examine whether patients shared genotypes. In addition, it compared the genotypes of the isolates from the same patients during two consecutive yrs.
METHODS
Patients
All seven Belgian CF centres participated in this study.
Sputum samples from a total of 276 P. aeruginosa-colonised CF patients were sent to the microbiology laboratory of the University Hospital of Ghent during 2003.
Sputum samples were mostly collected during an outpatient consultation, at the end of a physiotherapeutic session. This ensured that the samples originated from the deeper airways. When patients were too young or were unable to expectorate, a nasopharyngeal aspirate or swab was taken (26 nasopharyngeal samples taken versus 250 sputum samples). All centres were asked to send further sputum samples from the same patients 1-yr later. This sputum sample was obtained for a subgroup of 95 patients.
Patients were aged 5–54 yrs, mean±sd 24.2±8.8 yrs, and gave informed written consent. Approval was also obtained from the ethics committee of the University Hospital of Ghent.
Patients filled in a questionnaire (see Appendices 1 and 2) assessing the frequency and intensity of current and previous social contacts with other CF patients. CF sibling contacts were not taken into account. Scores assigned to the different possible answers in the questionnaire were agreed among the CF specialists involved in the study, whereby a subjective “weight” was given to the type of contact (for example an intimate relationship was scored as the highest risk factor for transmission (score 10) and occasional social contact as a minor risk factor (score 4)).
Of the patients from whom sputum P. aeruginosa was cultured, 93% completed the questionnaire.
Segregation policies are in place in all but one of the CF centres. In the outpatient clinics, P. aeruginosa-colonised patients and noncolonised patients are seen on different days. Care-givers are strongly advised not to wear jewellery and to wash their hands and stethoscopes between each visit. Patients are asked to wash their hands before lung-function measurement and to produce a sputum sample in a separate room. The filters of the lung-function testing equipment are always changed between patients. Patients with CF are always hospitalised in a single room and contact with other hospitalised CF patients is strongly discouraged.
These recommendations date from the mid-1990s and most centres implemented them in the succeeding years.
Microbiology
Sputum samples were inoculated onto McConkey agar (BBL Becton Dickinson, Cockeysville, MD, USA). After 2 days of incubation at 37°C, nonidentical-looking lactose negative colonies were picked, subcultured on 5% sheep blood agar (BBL Becton Dickinson) and tested for oxidase. Only oxidase-positive colonies were further identified, using transfer RNA intergenic spacer PCR (known as tDNA-PCR) 18.
Genotyping
For each patient, all P. aeruginosa isolates exhibiting each different colonial morphology on McConkey agar were first genotyped by arbitrarily primed PCR, using alkaline cell lysis for DNA-extraction and randomly amplification of polymorphic DNA (RAPD) analysis Ready-to-Go beads (Amersham Biosciences AB, Uppsala, Sweden) and primer ERIC2 (AAGTAAGTGACTGGGGTGAGCG) at an annealing temperature of 35°C, as previously described 18. This narrowed down the number of isolates that were subsequently genotyped by the more laborious fluorescent amplified fragment length polymorphism analysis (fAFLP; as previously described 19), since only single representatives of each RAPD-type were further genotyped by this procedure. The fAFLP-technique was described previously 19.
Statistical analysis
Measures of interpatient contact as obtained from the questionnaires did not approach a normal distribution (Kolmogorov-Smirnov Z-statistic p<0.001), therefore all analyses involving questionnaire scores were obtained under a nonparametric assumption. In order to assess putative differences in interpatient contacts between patients with a unique P. aeruginosa genotype and patients who shared at least one P. aeruginosa genotype with at least one unrelated patient, median “interpatient contact scores” were calculated for both groups and compared using the Median test. Dispersion of score values around a median value is presented as interquartile range (IQR). Differences in the distributions of score values between two groups were assessed with the Mann–Whitney U-test for two independent samples. Strength of association was expressed as (crude) odds ratios (OR) with 95% confidence intervals (CI) to the estimated OR. For any reported measure, statistical significance was accepted if the two-tailed probability level (p) was <0.05.
RESULTS
A total of 910 P. aeruginosa isolates from 213 patients out of 276 P. aeruginosa-colonised patients were genotyped using RAPD analysis. Further analysis using fAFLP was carried out only for single representative isolates from each group of isolates with the same RAPD-type. From 63 patients, no P. aeruginosa could be isolated, either because culture remained negative (n = 10), because technical problems occurred (n = 29) or because another Gram-negative organism was cultured (n = 24; six patients harboured Achromobacter xylosoxidans instead of P. aeruginosa, 15 patients harboured Stenotrophomonas maltophilia, one patient harboured both and two patients were colonised with Burkholderia cepacia).
After excluding isolates from the same patient with an identical RAPD pattern, 272 isolates from the patients, along with an additional three reference strains (epidemic strains from the UK: the Liverpool, Manchester and Midlands strains, provided by T. Pitt (Public Health Laboratory Service, London, UK)), were typed with fAFLP, a technique that is more reproducible than RAPD analysis and which yields digitised fingerprints. This allows large numbers of fingerprints to be compared by computer.
From the 213 patients’ 910 isolates, a total of 163 genotypes were found, based on fAFLP analysis. The majority of patients (160) had a single P. aeruginosa genotype, 48 patients had two genotypes and five patients had three genotypes (fig. 1⇓).
A limited number (13) of clusters, with “cluster” defined as a group of patients carrying P. aeruginosa isolates with the same genotype, was observed. There were three additional sibling clusters. The sizes of the clusters and their centre origins are listed in table 1⇓.
Sibling clusters excluded, 66 (30%) patients carried a P. aeruginosa isolate with a shared genotype. Five (2.3%) of these patients were part of two clusters.
There were six two-person clusters, one cluster of four patients, one of five patients, two of nine patients, two of 10 patients and one of 12 patients.
Of the 13 nonsibling clusters, 11 contained patients from more than one centre. In 10 out of 11 multicentre clusters, former contact between patients, such as a stay in a rehabilitation centre (rehabilitation centre A (rehab A) or rehabilitation centre B (rehab B)), attendance at a CF camp and/or social contact could be established.
When interpatient contact scores between cluster patients and noncluster patients were compared (100% of the cluster patients filled in their questionnaire versus 90% of the noncluster patients) a significant difference between the two groups was apparent (fig. 2⇓). Although the mean±sd age of both groups was comparable (24.7±9.1 yrs for the noncluster patients versus 23.2±8.2 yrs for the cluster group), the cluster patient group (n = 66) reported on average a significantly higher interpatient contact score than the noncluster group (n = 132; rank-sum p<0.001). The median (IQR) interpatient contact score of the cluster patients was 9.0 (5.0–14.0) versus 4.0 (0–7.0) for the noncluster patients.
During 2003, siblings (n = 24) invariably presented with at least one similar P. aeruginosa genotype at the level of the sibling pair (n = 12). Siblings represented 4.5% of the noncluster group of patients (six out of 132) compared with 27.3% of the cluster group of patients (18 out of 66; p<0.001), indicating that siblings are more prone to be involved in the spread of P. aeruginosa among CF patients (OR = 7.9; 95% CI = 3.0–21.0; p<0.001).
The latter observation might be explained by differential interpatient contact rates. Sibling patients (n = 24) reported on average a higher number of interpatient contacts than did unrelated patients (n = 174) with median (IQR) interpatient contact scores of 5.0 (4.0–14.0) and 4.0 (0.0–9.0), respectively, a difference that was marginally significant (p = 0.051) within the limits of the sample size.
Although the interpatient contact scores of siblings may actually be correlated data at the sibling pair level, the number of colonised siblings was too low in the current survey to assess and account for such a correlation and therefore the scores of all patients were handled as independent observations. To ensure, however, that a potential interaction at the sibling pair level did not bias the primary results in comparing the score values of the cluster and noncluster groups of patients, the analysis was repeated using only a single value each time for each sibling pair (a single mean score for each sibling pair, the lowest value of each sibling pair, and the highest value of each sibling pair, respectively). These analyses did not alter the current results.
None of the Belgian P. aeruginosa genotypes matched with the three UK strains.
For a total of 95 patients, sputum samples were collected in two consecutive years (2003 and 2004) and genotyped by fAFLP (fig. 3⇓). In total, identical P. aeruginosa genotypes were recovered from 76 (80%) patients in both years.
The genotypes that were newly acquired in 2004 were compared with the genotypes already present in the patient's CF centre in 2003. None of the “new” genotypes accorded with the known centre genotypes, except in one patient, whose novel genotype appeared to be identical to a genotype recovered from his sibling in 2003.
DISCUSSION
To the current authors’ knowledge, this study is the first to compare the P. aeruginosa genotypes of most colonised CF patients within one country. Most previous studies have examined the variety of genotypes within a centre 12, 14, 20–23.
The only comparable study was carried out in the UK 24, where a national survey was set up to identify and characterise transmissible P. aeruginosa strains in CF patients in England and Wales. Isolates were requested from >120 hospitals and a sample size of ∼20% of the CF population in each centre was attempted, but not always reached.
Different PCR fingerprinting techniques have been developed and different names have been used for identical techniques. Terms such as amplification fragment length polymorphism, arbitrarily primed PCR, DNA amplification fingerprinting or random amplification of polymorphic DNA are often used indiscriminately and create a “Tower of Babel” phenomenon. In a letter to the editor in the Journal of Clinical Microbiology in 2003, several CF physicians and microbiologists emphasised the need for harmonisation of techniques and technique designations for genotyping clinical isolates of P. aeruginosa from CF patients 25. Most of the epidemiological research studies 12, 16, 23 were based on pulsed field gel electrophoresis (PFGE).
Since the current authors’ laboratory had already built up experience of genotyping other species using RAPD and fAFLP 19, these techniques were used in the current study. This choice was supported by a study by Speijer et al. 26, which showed that fAFLP analysis was comparable with PFGE and RAPD analysis for P. aeruginosa isolates. D'Agata et al. 27 confirmed these findings.
Theoretically, it can be imagined that P. aeruginosa strains with slightly different fingerprints have only recently acquired mutations that make them differ from each other. As such, they may be clonally related, despite the differences in their fingerprints. The opposite can be true as well: strains with identical fingerprints can in reality differ from each other, because not all genomic differences are revealed by the fingerprint, which is obtained by looking at only some regions of the genome. When otherwise obvious differences exist in parts of the genome that are not addressed by the technique, these will be overlooked and the technique will yield identical fingerprints for genotypically different strains.
It can be stated, then, that genotyping studies are an approximation of the true genetic relatedness among the strains studied. However, whether cross-infection is underestimated owing to the fact that strains with slightly different fingerprints belong to the same genotype anyway is difficult to say, since overestimation as a consequence of genotypically different strains having coincidentally identical fingerprints is also possible.
However, Speijer et al. 26 showed that the clustering obtained using three different genotyping techniques (RAPD, fAFLP and PFGE), which address different regions of the genome, was concordant. Given the fact that the current authors also found concordance between fAFLP and RAPD in this and a previous study 19, it seems safe to assume that the present results reflect the true occurrence of genotypes and that there is neither under- nor overestimation of cross-infection.
For the 213 patients and 910 isolates tested, a total of 163 genotypes were found, indicating that different morphotypes in a single patient often have the same genotype.
This conclusion is supported by Hoogkamp-Korstanje et al. 28 and da Silva Filho et al. 20. A previous study 19 in a CF rehabilitation centre also found only 71 different P. aeruginosa genotypes among 749 isolates from 76 patients, indicating that in individual patients, isolates with different colonial morphologies mostly belonged to the same genotype.
In this national study, 75% of colonised patients carried P. aeruginosa of only one genotype during 2003. This corresponds with the findings of Mahenthiralingam et al. 29 and of the current authors’ previous study 19, where more than half of the patients (49 out of 76) carried only one genotype, 20 carried two genotypes and seven carried three genotypes.
In 24 out of 279 patients in the current study who had been thought to be colonised by P. aeruginosa, another Gram-negative organism was identified.
Some of the isolates, identified genotypically as Alcaligenes xylosoxidans or Strenotrophomonas maltophilia, seemed to be considered initially as atypical P. aeruginosa in routine laboratory analysis. Owing to the diversity of colonial morphologies and biochemical reactivity encountered, misdiagnosis of Gram-negative nonfermenters cultured from CF sputum may occur. In one study, misidentification of 11% of A. xylosoxidans strains was reported 30.
In a report about the occurrence of two large clusters of A. xylosoxidans in a CF rehabilitation centre population, the hospital laboratory initially misidentified this organism as P. aeruginosa 31.
Only a limited number of clusters (n = 13, plus three sibling clusters) were found by the current study, with a limited number of patients harbouring one of the P. aeruginosa cluster genotypes.
These findings were similar to data from the Vancouver CF centre 16 and the Brazilian study of da Silva Filho et al. 20.
Other centres, however, have reported large clusters with the same genotype. A study in a paediatric CF centre in Victoria, Australia 12 showed that 55% of the 118 P. aeruginosa-colonised CF children carried the same genotype and the Manchester, UK CF centre 9 had to deal with a multi-resistant strain carried by 14% of its 154 P. aeruginosa-colonised patients. In the Liverpool, UK CF centre 8 60% of 92 P. aeruginosa-colonised children harboured the same strain.
A Norwegian study 11 showed that only seven out of 60 patients carried a distinct P. aeruginosa genotype, the rest being made up of one large main cluster of 27 patients (45%) and further clusters of two to four patients. Patients were known to have contact during holiday camps and training courses.
In the nationwide survey of Scott and Pitt 24, 72% of patients harboured strains with unique genotypes, a proportion that matches the results of the current study. In their study, small clusters of related strains were evident in some centres, presumably indicating limited transmission of local strains. The most prevalent strain (“Liverpool” genotype) accounted for 11% of patient isolates from 15 out of the 31 examined centres. The second most prevalent strain (“Midlands1”) was recovered from 86 patients in nine centres and clone C (originally described in Germany) was found in 15 patients from eight centres. A fourth genotype, identical to the “Manchester” strain, was found in three centres.
The Liverpool, Manchester and Midlands strains were not detected in the Belgian CF population. The present data did not point to a Belgian “problem” genotype, carried by many patients, since the largest cluster contained only 12 patients (5.5% of the studied population).
It is not known whether these cluster genotypes are multi-drug resistant, since susceptibility testing was not performed during this study.
In the present study, most clusters, (11 out of 13) contained patients from different CF centres. The vast majority of these patients had spent time in one of the two Belgian rehabilitation centres (rehab A and rehab B), or had participated in a CF camp. At least two patients had shared a hospital room with another nonsibling CF patient.
The largest cluster of 12 patients (cluster four), contained six patients who had stayed several years ago in rehab B and four patients who had stayed in rehab A, while the remaining two patients were siblings who had stayed in both centres for prolonged periods. It is possible to speculate that this sibling pair caused the spread of this cluster genotype. In cluster six, eight out of the 10 patients had stayed in rehab A. The clustering of the isolates from the remaining two patients remains unexplained, since they had never stayed in rehab A, and since they mentioned close contacts with each other, but not with others from cluster six.
Three out of the five patients in cluster eight had been on a CF holiday camp (two of them could not specify which camp and when, since these camps took place >10 yrs ago).
One two-person cluster (cluster 13) contained two young schoolchildren, followed at the same CF centre. These girls were close friends, and, though they were discouraged from doing so, they always came to the centre together, in the same car. They went to the same physiotherapist, shared the same classroom and even wanted to be hospitalised together. In these two children, it was obvious that patient-to-patient transmission had occurred (within the setting of an in- and outpatient CF clinic).
Since segregation between P. aeruginosa-colonised and noncolonised patients has been installed in almost all Belgian CF centres (except for centre B) and rehabilitation centres since the mid-1990s, any other patient-to-patient transmission is suspected to have occurred before that period.
In a previous study in one of the two Belgian rehabilitation centres 19, during 2002 and 2003, 38 out of 45 patients with a cluster strain already carried this strain upon arrival at the CF centre. Therefore, the possibility that acquisition of this strain from a common source, or from another patient, occurred during a previous stay in the CF centre, before more stringent infection control measures were introduced, could not be excluded.
The earlier study could establish that the risk of patient-to-patient-transmission during the study period was relatively low (10%), and that the risk of persisting colonisation with a newly acquired strain during the study period was still lower (4%).
In the current study, siblings carried the same P. aeruginosa genotype. The current authors did not take into account the sibling clusters, nor were sibling contacts covered in the questionnaire, since it could be considered as “obvious” that siblings would share genotypes 13, 32, 33.
In the current Belgian cohort study, siblings (n = 24) represented 4.5% of the noncluster group of patients (six out of 132) compared with 27.3% of the cluster group of patients (18 out of 66; p<0.001) suggesting that siblings are much more prone to be involved in the spread of P. aeruginosa among CF patients (OR = 7.9; 95% CI = 3.0–21.0; p<0.001).
It is possible to speculate that siblings stay in rehabilitation centres more often than nonsiblings, because the burden of having two children with CF (and having to devote a lot of time to their treatment) “forces” parents to send their children to these centres from time to time.
It is also possible that siblings are more willing to stay in a rehabilitation centre or to attend a holiday camp, since they don't have to go alone (in contrast with nonsibling patients).
In a subgroup of 95 patients, P. aeruginosa genotyping was performed in two consecutive years. The vast majority (80%) continued to carry their own predominant strain. Of those patients who had a “new” genotype in 2004, only one had a genotype that matched a genotype from the patient’s own centre in 2003. The strain with the matching genotype, however, had been isolated from the patient’s sister in 2003. It is possible that this strain was already present in the patient during 2003, but was overlooked, or that it had been acquired from the patient’s sister in the period between samplings. Since no other “new” genotypes in 2004 seemed to match the “known centre genotypes” of 2003, it seems likely that patient-to-patient transmission did not occur within the Belgian centres for this subgroup of patients.
A limitation of the study is the lack of validation of the questionnaire. As mentioned previously, the scores were arbitrarily assigned, since no other scoring system, evaluating the amount and intensity of social contacts, has been used in CF studies.
Although this scoring system remains subjective, the questionnaire enabled the current authors to assign to some degree an interpatient contact score to each patient.
In conclusion, the present findings confirm that, in the Belgian cystic fibrosis population, different colonial morphotypes of Pseudomonas aeruginosa from a single cystic fibrosis patient usually belong to the a single genotype. Genotypic diversity among Pseudomonas aeruginosa strains is large in Belgian cystic fibrosis patients. The current authors could describe only a limited number of clusters. The situation varies from one country to another and probably depends on multiple factors such as the number of patients per centre, the presence of highly transmissible strains and segregation measures. Most clusters in the present study could probably be explained by previous social contacts (mostly during previous stays in rehabilitation centres and holiday camps). The majority (80%) of a subgroup of patients continued to carry its own predominant strain during two consecutive years, suggesting a small genotype variability per patient, despite the large genotype diversity in the population.
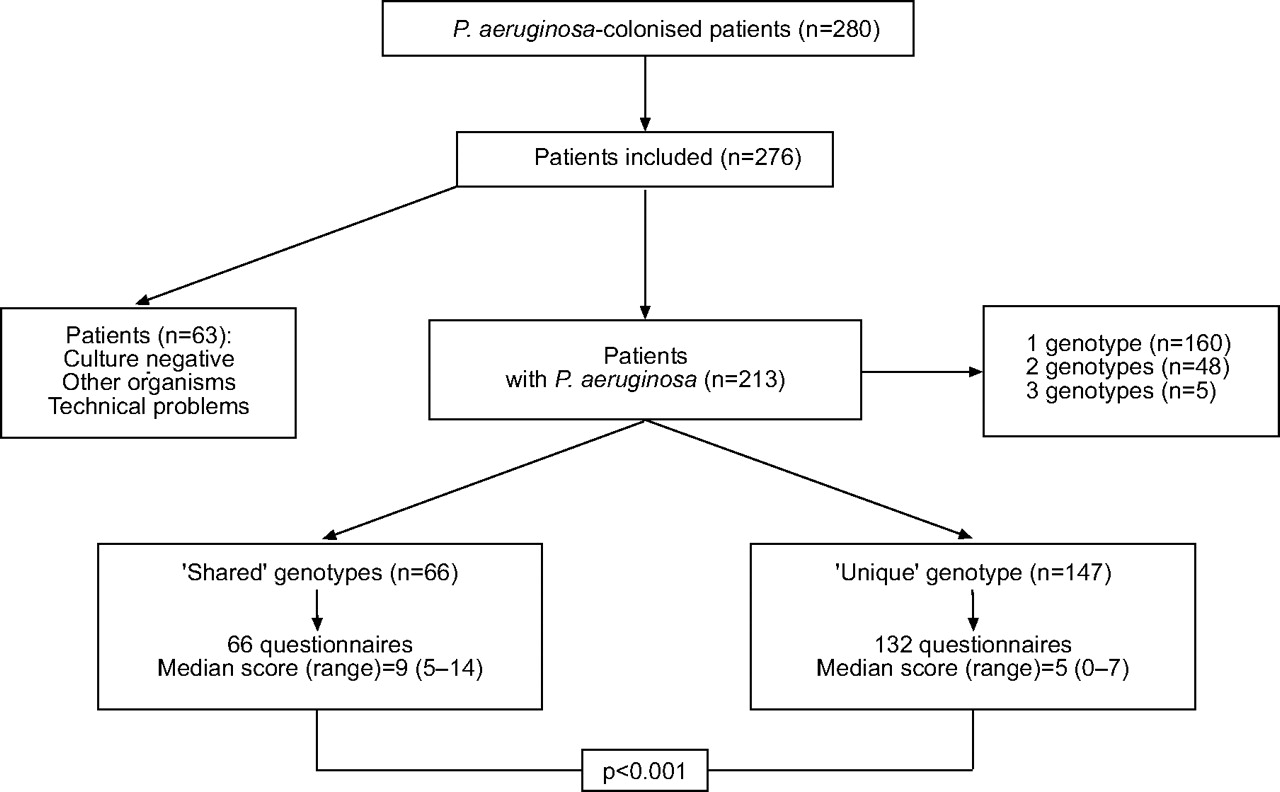
Flow chart of the study design and of the Pseudomonas aeruginosa genotyping results.

Interpatient contact scores of patients with a unique Pseudomonas aeruginosa genotype (noncluster patients) compared with those of patients sharing a P. aeruginosa genotype with at least one other unrelated patient (cluster patients). Data are presented as median, interquartile range and range.

{kind=link}
{kind=link}
{kind=link}
Comparison of the Pseudomonas aeruginosa genotypes of 95 patients, sampled during both 2003 and 2004.
Pseudomonas aeruginosa genotypes shared in Belgian cystic fibrosis patients
Appendix 1: Questionnaire for parents of CF patients <14 yrs of age
1. Does your child have contact with other CF patients in the family, other than brothers or sisters (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 8.
2. Does your child have contact with other CF patients in the classroom (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 7.
3. Does your child have contact with other CF patients at school (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 4.
4. Did your child ever stay in a rehabilitation centre? YES/NO. If yes, in which rehabilitation centre and for how long? YES = score 5.
5. Did your child ever attend a CF camp? YES/NO. If yes, which camp and for how long? YES = score 5.
6. Has your child ever shared a hospital room with another CF patient (brothers and sisters excluded)? YES/NO. If yes, with whom (initials only)? YES = score 5.
7. Does your child have social contacts with other CF patients (excluding contacts already asked for in previous questions)? YES/NO. If yes, with whom (initials only)? YES = score 4.
TOTAL SCORE =
Remark 1: “social contacts” are “physical” contacts (playing, talking, etc.), not written or internet contacts! Remark 2: you are not obliged to answer these questions if you don't want to. Remark 3: this questionnaire is sent to the investigating lab in a sealed envelope.
The members of your CF centre will not be able to look at the answers.
Appendix 2: Questionnaire for adolescents and adults with CF
1. Do you have contact with other CF patients in the family, other than brothers or sisters (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 8.
2. Do you have contact with other CF patients in the classroom (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 7.
3. Do you have contact with other CF patients at school or at work (now or in the past)? YES/NO. If yes, with whom (initials only)? YES = score 4.
4. Have you ever had a sexual relationship with another CF patient? YES/NO. If yes, with whom (initials only)? YES = score 10.
5. Did you ever stay in a rehabilitation centre? YES/NO. If yes, in which rehabilitation centre and for how long? YES = score 5.
6. Did you ever attend a CF camp? YES/NO. If yes, which camp and for how long? YES = score 5.
7. Have you ever shared a hospital room with another CF patient (brothers and sisters excluded)? YES/NO. If yes, with whom (initials only)? YES = score 5.
8. Do you have social contacts with other CF patients (excluding contacts already asked for in previous questions)? YES/NO. If yes, with whom (initials only)? YES = score 4.
TOTAL SCORE =
Remark 1: “social contacts” are “physical” contacts (talking, going out together, etc.), not written or internet contacts! Remark 2: you are not obliged to answer these questions if you don't want to. Remark 3: this questionnaire is sent to the investigating lab in a sealed envelope.
The members of your CF centre will not be able to look at the answers.
Acknowledgments
The authors would like to thank the CF nurses M. Vanderkerken, L. Boulanger, J. Birchall, C. Vandekerckhove, A. Beaudelot, F. de la Colette, E. Vanlanghendonck and E. Cooreman for their help in this study, H. Verstraelen for statistics and L. Van Simaey for laboratory work.
- Received January 9, 2006.
- Accepted May 12, 2006.
- © ERS Journals Ltd
References










