





Abstract
Statins inhibit the 3‐hydroxy‐3‐methylglutaryl coenzyme A reductase, reduce the serum level of low-density lipoprotein cholesterol, and are extensively prescribed to prevent cardiovascular mortality and morbidity. Few systemic adverse effects, such as pseudopolymyositis, lupus-like syndromes, and anecdotal hypersensitivity pneumonitis, have been reported.
A simvastatin-induced diffuse interstitial pneumonia associated with a nonspecific interstitial pneumonia pattern at histological analysis is repoted here. Ultrastructural analysis showed a diffuse cytoplasmic accumulation of intralysosomial lamellar inclusions in type II pneumonocytes, histiocytes and endothelial cells, suggesting a shared pathogenesis with amphiphilic drug-induced toxic lung injury. Because statins are increasingly prescribed, statin-induced interstitial lung disorders may be more frequently observed and early recognition will be required.
Statins are highly efficient in preventing both cardiovascular morbidity and mortality 1. However, several cases of lupus-like or pseudodermatopolymyositis syndromes have been reported 2–6. Although pulmonary adverse side-effects are also frequently suspected, observations are rarely supported by histological data. When open lung biopsies are performed, a pattern of hypersensitivity pneumonitis with granulomas is usually described 5, 6.
A case of statin-induced lung injury, with a histological pattern of nonspecific interstitial pneumonia (NSIP) is reported here. The ultrastructural analysis showed lamellar intralysosomial inclusions in the cytoplasm of pneumonocytes, macrophages and endothelial cells, suggesting that as well as the classical hypersensitivity pattern, an amphiphilic drug-like toxicity might account for simvastatin lung injury.
Case report
A 51‐yr-old male with a history of myocardial infarction related to severe coronary heart disease was admitted for fever, polymyalgia, cough and progressive dyspnoea for 1 month. He had a noninsulin-dependant diabetes mellitus and was treated with glibenclamide (10 mg·day−1), betaxolol (20 mg·day−1), and simvastatin (5 mg·day−1) for 6 yrs. Chest examination revealed fine rales, consistent with bilateral and diffuse infiltrates on chest radiography, and ground-glass opacities, with focal areas of condensation at the lung bases on the computed tomography (CT) scan (fig. 1⇓). The results of laboratory tests were normal except for a mild peripheral eosinophilia (500·mm3), an elevation of both creatine phosphokinase (430 UI·L−1) and C‐reactive protein levels (140 mg·L−1). Arterial blood gas measurements revealed the following: pH 7.46; oxygen tension in arterial blood (Pa,O2), 9 kPa; and carbon dioxide tension in arterial blood (Pa,CO2), 4.1 kPa. Pulmonary function tests revealed a restrictive ventilatory pattern with decreased diffusing capacity (forced vital capacity (FVC), 2.81 L (65% of predicted); forced expiratory volume in one second (FEV1), 2.17 L (63% pred); FEV1/FVC 77%; and diffusing capacity of the lung for carbon monoxide, 33% pred). Fibreoptic bronchoscopy demonstrated normal airways, and bronchoalveolar lavage (BAL) revealed a white blood cell count of 674 cells·µL with 64% of lymphocytes (89% of CD8+ T‐cells). Because a drug-induced pneumonitis was highly suspected, betaxolol and simvastatin were discontinued and a corticosteroid therapy (1 mg·Kg−1/day−1) was added.

Lung computed tomography scan showing bilateral interstitial infiltrates with ground-glass opacities predominating in the lower lobes.
One month later, symptoms and chest radiography were not improved, and an open lung biopsy was performed. The histological analysis showed a diffuse involvement of the interstitium preserving the lung architecture, with a temporal uniformity (fig. 2⇓). In some subpleural areas, fibrosis was more prominent with focal scarring concerning <10% of the parenchyma on the biopsy. Alveolar walls were thickened by a mixed inflammatory infiltrate, predominantly of lymphocytes and plasma cells with a mild fibrosis. Neither peribronchiolar inflammation nor granuloma formation were observed, and airspaces were filled by foamy macrophages. Similar foamy cytoplasmic abnormalities were present within hyperplastic type II pneumonocytes and interstitial histiocytes. Overall features were consistent with the diagnosis of a fibrotic NSIP. Ultrastructural analysis revealed heterogeneous intralysosomial lamellar inclusions in the cytoplasm of type II pneumonocytes, interstitial histiocytes and endothelial cells, suggesting a phopholipidosis (fig. 3⇓).
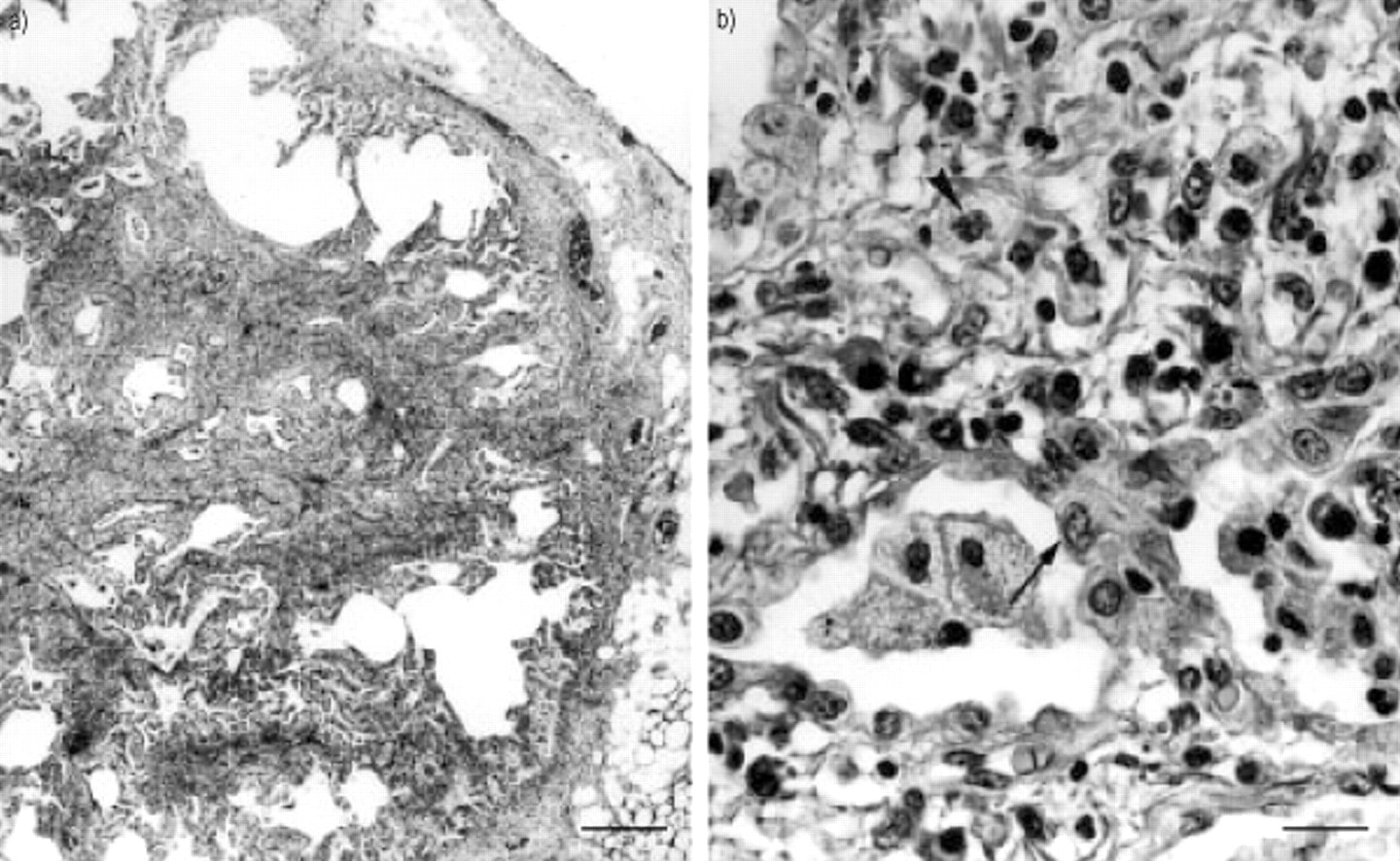
a) Subpleural area with focal honeycombing (internal scale bar=100 microns). b) Hyperplastic type II pneumonocytes (arrow) lining the alveolar walls and interstitial histiocytes (arrowhead) both presenting a foamy cytoplasm (internal scale bar=10 microns).

Electron microscopy revealing heterogeneous intralysosomial lamellar inclusions in the cytoplasm of pneumonocytes (internal scale bar=1 µm).
Six months later, a progressive response to corticosteroid therapy was observed with improvement of both respiratory symptoms and lung infiltration on chest radiography. One-month later, pravastatin was inadvertently introduced, and rapidly followed by an elevation of creatine phophokinase, an increase of dyspnoea and myalgia and new infitrates on chest radiography. Statin was rapidly stopped, leading to a progressive clinical and radiographical improvement.
Discussion
Statins are the most frequently prescribed lipid-lowering drugs, which allow for a significant decrease in cardiovascular mortality 1, whilst also being associated with a low frequency of side-effects. Statins inhibit the 3‐hydroxy‐3‐methylglutaryl (HMG‐CoA) reductase, mimicking their substrate HMG‐CoA, and curtail the formation of mevalonic acid metabolites, including cholesterol. In addition, statins increase the expression of the low-density lipoprotein (LDL) hepatic receptors, leading to a reduction in the LDL serum levels and the synthesis of new LDL 7. The most frequent side-effects are cataracts, myopathy, rhabdomyolysis, and augmentation of hepatic enzyme levels, while the incidence of pseudopolymyositis syndromes is low (0.1%) 6.
Statin-related hypersensitivity pneumonitis has been previously reported, using either pravastatin, lovastatin or simvastatin 6. Histological analysis showed a classical, patchy distribution of the alveolitis with an early granuloma formation, and a diffuse fibrosis of the alveolar walls 5, 6. An NSIP has never been described in statin-induced lung injury, which is classically related to amiodarone 8. Idiopathic and drug-related NSIP share a similar histological presentation, with a mixture of inflammation and fibrosis of the interstitium and a temporal uniformity of the lesions, which are the hallmarks of this entity 9. However, areas of organizing pneumonia or rare, poorly formed non-necrotizing granulomas have also been described in NSIP, suggesting that hypersensitivity pneumonitis may be an early stage of the inflammatory process, which promotes the subsequent development of NSIP 10. In the present study, despite an absence of histological criteria for a hypersensitivity pneumonitis, the presence of a large amount of alveolar CD8+ T‐cells, a peripheral eosinophilia and the clinical worsening accompanying statin reintroduction supported the argurment of the potential role of a hypersensitivity in the pathogenesis of NSIP 11, 12.
The NSIP pattern differs from usual interstitial pneumonia through the absence of numerous fibroblastic foci and areas of honeycombing in subpleural and paraseptal location besides normal lung 9. However, with the recent distinction of cellular and fibrotic variants, interstitial collagen deposition corresponding to old scarring may also be observed in NSIP. This latter pattern was associated with a weaker response to corticosteroid therapy 10, and might explain the slow and partial resolution of the process after drug discontinuation and corticosteroid therapy introduction in this case.
The pathogenesis of amphiphilic drugs-related lung injury remains largely controversial. It may be dependant on both immunological and toxicological mechanisms 13, 14. The ultrastructural analysis of amiodarone-induced pneumonitis has demonstrated the presence of intralysosomial lamellar inclusions in pneumonocytes and in interstitial cells 15, 16. It is hypothesized that there is a toxic mechanism, possibly mediated by the inhibition of phospholipidases, leading to cellular accumulation of intralysosomial phospholipids 16, 17. Similarly, in statin-induced lung pneumonitis, the mechanisms of injury remain unknown. The identical description of intralysosomial lamellar inclusions in pneumonocytes and in interstitial cells is highly suggestive of an effect upon lipid metabolism. However, whether it is a direct toxic effect or an indirect toxic effect related to the activation of an inflammatory immune response, needs to be clarified.
As well as the classical effectiveness of statins as lipid-lowering drugs in the treatment of cardiovascular disease 1, new properties have been described. Statins may also be of interest in the reconstruction of bone matrix and in the treatment of osteoporosis 18. Thus, a higher number of patients might develop pulmonary side-effects. In addition to the more classical hypersensitivity pneumonitis, a fibrotic nonspecific interstitial pneumonia should henceforth be considered. Whereas hypersensitivity pneumonia usually shows a good response to corticosteroid treatment, the presence of a fibrotic process may be associated with slow and partial responses, accounting for a less favourable prognosis.
- Received July 6, 2001.
- Accepted August 1, 2001.
- © ERS Journals Ltd










{kind=link}
{kind=link}
{kind=link}