





To the Editors:
Inflammatory myofibroblastic tumour (IMT) is a relatively uncommon lesion and occurs in nearly every site of the body. Patients with IMT are usually asymptomatic, with a solitary nodule or mass detected by routine chest radiograph 1. Many diagnostic procedures can be applied to make the diagnosis: computed tomography (CT) scan to outline nodule growth and perfusion, [18F]-2-fluoro-deoxy-D-glucose (FDG)-PET/CT scan to evaluate metabolic activity and 111In-Diethylene triamine pentaacetic acid (DTPA)-D-Phe1 scan (octreoscan) to investigate somatostatin analogue receptors, often present in a variety of neuroendocrine tumours (NETs).
We present two cases of pulmonary IMT clinically misdiagnosed as carcinoid tumours due to a positive octreoscan.
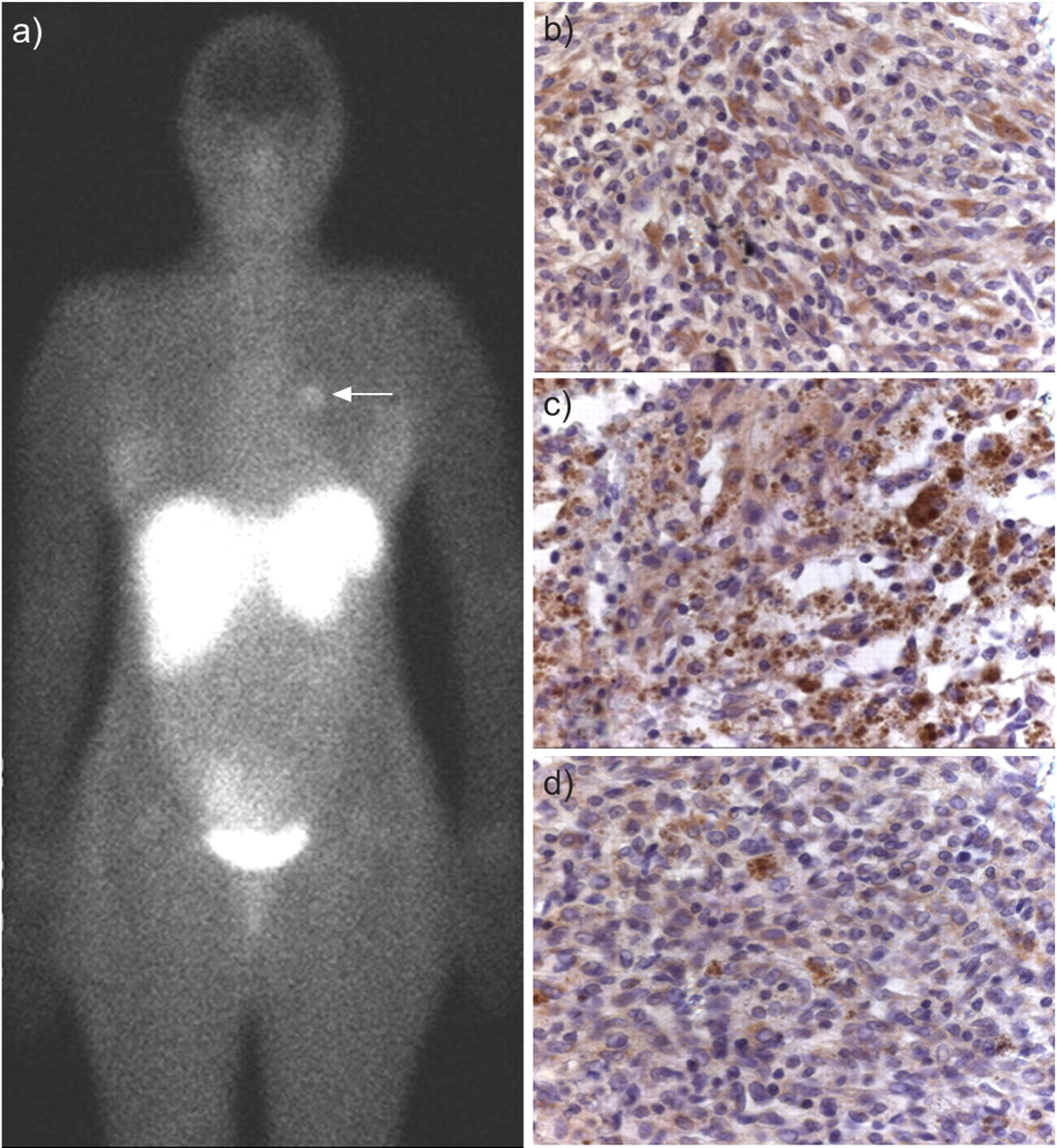
Case 1 was a 52-yr-old female former smoker who was admitted to our hospital with thoracic pain. The electrocardiogram was completely negative for angina or myocardial infarction. Chest radiograph and CT revealed a left hilar nodule, sharply circumscribed, slightly lobulated, with a mild homogeneous increase of density after enhancement. A whole-body FDG-PET/CT scan showed increased tracer uptake of the lung mass (standardised uptake value (SUV) 25) compatible with a malignant lesion. SUVmax was calculated 50 min after injection and normalised for body weight. After intravenous administration of 111 mBq of [111In]-octreotide, an abnormal, although low, uptake was present in the left lung hilar region (fig. 1a⇓). Bronchoscopy was negative. On the basis of the CT, FDG-PET/CT and octreoscan, a clinical/radiological diagnosis of a carcinoid tumour, most probably atypical, was postulated. The intraoperative frozen specimen excluded the diagnosis of a carcinoid tumour and the lesion was regarded as a low-grade spindle cell malignancy. A left upper lobectomy with complete lymph node dissection was performed. Tumour size was 3 cm in the greatest diameter, circumscribed and yellowish on the cut surface. Microscopically the lesion consisted of spindle cells arranged in a storiform pattern and an admixture of inflammatory cells, with a predominance of histiocytes and lymphocytes. The spindle cells had low cellular atypia and no mitotic activity. Immunohistochemical findings are reported in table 1⇓ and somatostatin receptor (SSTR)2A, SSTR3 and SSTR5 staining is shown in figures 1b–d⇓. The final diagnosis was IMT. The post-operative course was unremarkable and the patient was discharged from the hospital after 8 days.

{kind=link}
(Case 1). Octreoscan uptake in the left hilar region of the lung (a) and immunohistochemistry for SSTRs: scattered neoplastic spindle cells and inflammatory cells strongly marked are well seen (b: SSTR2A, c: SSTR3, d: SSTR5. Original magnification: x 200).
Antibody findings
Case 2 was a 31-yr-old male former smoker who was admitted to our hospital with a 3-month history of dry cough, low-grade fever, clubbing and bilateral knee, ankle joint stiffness, anaemia and increased erythrocyte sedimentation rate. Past history showed that both a thorough microbiological and immunological analyses were negative. Chest radiograph and CT scan with contrast enhancement revealed a left lower lobe round-shaped solitary lesion with sharp margins, slight inhomogeneous hypodensity and mild, homogeneous enhancement uptake. Bronchoscopy was normal and a whole-body FDG-PET/CT scan revealed a lesion with high hypermetabolism (SUV: 22). SUVmax was measured as described in case 1. Octreoscan showed high tracer uptake of the pulmonary mass. A proposed diagnosis of carcinoids (perhaps atypical) was made.
The patient underwent a left lower lobectomy with complete lymph node dissection. On gross examination, the tumour size was 4 cm in the greatest diameter, well circumscribed and greyish on the cut surface. At histology, the lesion demonstrated marked cellular proliferation of spindle cells with admixed inflammatory cells mainly represented by plasma cells, lymphocytes and macrophages. Immunohistochemical findings are reported in table 1⇑. The final diagnosis was IMT. The post-operative course showed quick resolution of the systemic symptoms and signs, and the patient was discharged after five days.
IMT is a generic term used for a variety of neoplastic and non-neoplastic entities that have a common histological feature characterised by bland spindle cell proliferation with a prominent, usually chronic, inflammatory infiltrate.
The old concept of Matsubara et al. 2 which considered most cases of IMT a result of an aberrant repair reaction has now been changed. Since the 1990s, IMT has become known as a distinct entity with peculiar clinical, pathological and molecular characteristics. Under the current classification IMTs are considered to be myofibroblastic; however, smooth muscle actin positivity and other markers of myofibroblastic differentiation cannot always be demonstrated. Macrophage-dendritic cell markers have been reported in different series 3 suggesting that IMT may also be considered a proliferative disorder of these cell lines. Thus, as reported by Farris et al. 4, the term “inflammatory myfibroblastic tumour” is a misnomer in ∼50% of cases.
Flow cytometry studies have found aneuploid (hyperploid) indices in IMT, leading to the suggestion that it is a neoplasm. Multiple chromosomal abnormalities have been detected in IMT most notably involving the ALK locus on chromosome 2p23. Clonal abnormalities of ALK are usually detected in 50–60% of anaplastic large cell lymphomas providing further support for the neoplastic nature of IMT. The expression of ALK1 and p80 are reported in ∼40% of IMT cases 1. Reactivity for p53 has been detected with variable frequency (from <10% to 80%) and its association with recurrence and malignant transformation has been largely debated 1.
The lungs are frequently involved but the incidence is reported to be <1% of all lung tumours. Symptoms are related to tumour localisation; however, many cases are asymptomatic 1. Of the cases reported in the literature only 19% were accompanied by some type of systemic symptoms such as fever, anaemia and increased erythrocyte sedimentation rate 5 as were present in one of our reported cases. Previous studies have demonstrated overproduction of large amounts of pro-inflammatory cytokines such as tumour necrosis factor α, interleukin (IL)-6 and IL-3; which could be responsible for many systemic symptoms 6. The prognosis of patients with resected IMT is excellent: 78–100% of patients were in complete remission after an average follow-up of 3.3 yrs. Intrathoracic recurrence was reported in 5% of cases and metastasis occurs in <5% of cases 1.
The radiological differential diagnosis for IMT occurring as a solitary pulmonary nodule includes primary or secondary neoplasms, haemartoma, chondroma, and granuloma.
In our cases, the patients were studied by conventional chest radiograph, CT, FDG-PET/CT and octreoscan. Few works have described the use of FDG-PET/CT in IMT, reporting different ranges of SUV values (from 5 to >35) 7, 8. A larger number of cases could provide strategic information on clinical and morphological/molecular phenotypes. The positive findings of the octreoscan in our cases are related to the immunohistochemical detection of SSTRs on all tumour cell components, either spindle or inflammatory cells. SSTRs are largely expressed in NETs and represent the molecular basis for the clinical use of somatostatin analogues in treatment of NETs and their in vivo localisation. SSTR subtype expression has been detected in other different types of human tumours 9 and in non-neoplastic lesions, particularly immune-mediated diseases such as rheumatoid arthritis, Graves' disease, tuberculosis and sarcoidosis 10. To our knowledge, these are the first documented cases of IMT with positive octreoscan and SSTR immunohistochemistry.
In summary, IMT should be kept in mind when ruling out a diagnosis of a solitary pulmonary nodule, even in cases with positive octreoscan results.
A combination of clinical information, CT, FDG-PET and octreoscan findings could lead to a more precise diagnostic characterisation of pulmonary nodules. Moreover, the confirmation of such findings in larger case series may also give new insights for a targeted therapy.
Statement of interest
None declared.
- © ERS Journals Ltd
References










