





Abstract
Pseudomonas aeruginosa is an important pathogen in cystic fibrosis (CF). Although most patients harbour unique P. aeruginosa isolates, some clinics report patients sharing common strains. The overall importance of person-to-person transmission in P. aeruginosa acquisition and whether routine patient segregation is necessary remains uncertain. The present authors therefore investigated the extent of P. aeruginosa transmission in New Zealand CF clinics.
New Zealand’s seven major CF centres were assessed, combining epidemiological data with computer-assisted SalI DNA fingerprinting of 496 isolates from 102 patients.
One cluster of related isolates was significantly more prevalent in the largest clinic than expected by chance. The seven patients with isolates belonging to this cluster had more contact with each other than the remaining patients attending this centre. No other convincing evidence of transmission was found in any of the other smaller clinics. Three P. aeruginosa strains believed to be transmissible between patients in Australian and British CF clinics are present in New Zealand, but there was no definite evidence they had spread.
Pseudomonas aeruginosa transmission is currently infrequent in New Zealand cystic fibrosis clinics. This situation could change rapidly and ongoing surveillance is required. The current results confirm that computer-assisted SalI DNA fingerprinting is ideally suited for such surveillance.
Once Pseudomonas aeruginosa is established within the lungs of patients with cystic fibrosis (CF) there is an accelerated decline in pulmonary function, quality of life and life-expectancy 1. Most CF patients acquire P. aeruginosa strains from environmental sources 2. However, siblings are often infected with indistinguishable clones suggesting person-to-person transmission instead of common environmental exposure 3. Furthermore, in several European, English and Australian CF clinics, many patients share a common strain 2, 4–7. Some strains appear in several clinics 8, 9, others superinfect patients already chronically colonised with unrelated P. aeruginosa isolates 10, while some are associated with worse outcomes and increased treatment costs 6, 7, 11–13. In contrast, others have found only small clusters of genetically similar isolates from CF patients lacking geographic or temporal relationships other than attending the same clinic 14–16. Rather than from cross-infection, such clusters could be due to common environmental sources or limited discriminatory power of typing methods 17.
Consequently, P. aeruginosa transmission between CF patients may occur, but only after prolonged close contact, as in siblings, or from small numbers of strains with heightened potential for transmission. Nonetheless, British and, more recently, Australian CF Trust infection control guidelines and the European consensus report recommend that all CF patients with P. aeruginosa be segregated to reduce cross-infection [18–20]. Centres in Australia and Europe that implemented these recommendations have been successful at restricting potentially transmissible strains 21, 22. However, segregation-based infection control policies are expensive and difficult to implement, and adversely affect patient well-being without reducing sporadic P. aeruginosa acquisition 22. It is therefore important to determine whether cross-infection is occurring within individual clinics.
Previously, a computer-assisted DNA fingerprinting method was described, which is simple, fast and cost-effective 23. The DNA fingerprints are stable 23, the pattern score-based genetic distances correlate with DNA sequence-based genetic distances 23, and its discriminatory power matches that of pulse-field gel electrophoresis (PFGE), the current gold standard for molecular typing P. aeruginosa isolates 23–25. A robust pattern scoring system used with the DNA fingerprinting technique largely overcomes problems associated with noncategorical molecular typing methods 17. Previously, using computer-assisted SalI fingerprinting, indications of possible transmission in one New Zealand clinic were found based upon P. aeruginosa isolates from CF patients being genetically less diverse than isolates obtained from patients without CF 23. However, it was not directly established that this resulted from CF clinic attendance. Therefore, a multi-centre study was conducted to determine the likelihood of P. aeruginosa transmission in New Zealand CF clinics by combining epidemiological data with SalI fingerprinting. The clinics were located in cities 100–1,100 km apart. Each employed standard hygiene methods, but most had not implemented patient segregation.
METHODS
Patients, data collection and isolates
Participants attended one out of seven (table 1⇓) clinics caring for 269 CF patients (102 adults aged ≥15 yrs; clinic size 21–57), representing 71% of child, 84% of adult and 75% of total New Zealand CF patients. Treatment and infection control protocols were similar between hospitals 26. Inpatients were nursed either in single rooms with their own bathrooms or in wards with non-CF patients. Contact between CF patients was discouraged and respiratory equipment was not shared. In-line filters, mouthpieces and connectors for pulmonary function equipment were discarded or sterilised after use, and physiotherapy was conducted separately. Segregation of all CF individuals in outpatient clinics was practised by Starship Children’s Health (Auckland), Christchurch Hospital (paediatric clinic only; Christchurch) and Dunedin hospitals (Dunedin, New Zealand). The other hospitals segregated only those harbouring Burkholderia cepacia complex or methicillin-resistant Staphylococcus aureus. The Ministry of Health’s Multi-Region Ethics Committee (Wellington, New Zealand) approved the study as a clinical audit.
Patient population and isolates
Following informed consent, single sputum or oropharyngeal specimens were collected from CF patients attending routine clinic appointments between July 2004 and August 2005. The patient’s physician entered centre, age, sex, sputum microbiology and, for the previous 12 months, dates of hospitalisation and clinic attendances, best recorded body mass index (BMI) z-scores and forced expiratory volume in one second (FEV1) % predicted values into a secure database.
Respiratory samples were inoculated on selective media to detect CF respiratory pathogens by standard techniques 27. When P. aeruginosa was identified, five randomly selected colonies were each inoculated into glycerol broth and stored at -70°C (see online supplementary material).
Representative isolates of clonal strains from CF patients in Liverpool 4 and Manchester 5 (both UK) and Melbourne (two pulsotype1 isolates) 6 and Brisbane (pulsotype2; both Australia) 7 were kindly provided by J. Govan, University of Edinburgh (Edinburgh, UK), A. Jones, Manchester Adult CF Centre (Manchester, UK), D. Armstrong, Monash University (Melbourne, Australia) and S. Bell, the Prince Charles Hospital (Brisbane, Australia), respectively.
P. aeruginosa genotyping
DNA fingerprinting was performed as described previously 23. Briefly, following electrophoresis and ethidium bromide staining of SalI digests of genomic DNA, the number of restriction fragments in molecular weight brackets (defined by an XV molecular weight standard (Roche Diagnostics, Auckland, New Zealand) loaded in alternate lanes) was counted for each strain, and used to calculate genetic distances (see online supplementary material). Distances were displayed as unweighted pair-group method with arithmetic mean (UPGMA) trees using Paup*4.0 (Sinauer Associates, Sunderland, MA, Australia). Five colonies per patient were typed. PFGE of SpeI-genomic DNA digests of P. aeruginosa isolates was also performed 28.
Statistical analysis
Simple descriptive statistics, binomial, unpaired t- and Fisher’s exact tests were performed. Statistical significance was determined by p<0.05 and Bonferroni correction applied when multiple comparisons were made.
RESULTS
Frequency of P. aeruginosa in the study population
Out of the 269 patients attending seven clinics, 102 (38%) had P. aeruginosa in sputum (n = 97) or oropharyngeal (n = 5) cultures. The characteristics of these 102 patients are shown in table 2⇓.
Characteristics of patients withPseudomonas aeruginosa
Evidence for transmission at one centre
Table 1⇑ shows that 496 P. aeruginosa isolates from 102 CF patients underwent DNA fingerprinting. This included two patients who moved during the study and provided samples in two clinics. Table 1⇑ also displays the degree of contact between patients. Figure 1⇓ shows the relationships between isolates as a UPGMA tree. If a patient had several isolates with identical patterns, only one of these is included in the tree. Four strains highly prevalent in CF clinics overseas are also included.

Unweighted pair-group method with arithmetic mean tree based on SalI pattern score-based genetic distances between representative isolates (where multiple isolates from the same patients are scored as identical, only one representative is included). Isolate labels reflect the clinic in New Zealand at which a patient was treated (Greenlane (GRE; Auckland); Starship (STA; Auckland); Waikato (WAI; Hamilton); Palmerston North (PAL); Wellington (WEL); Christchurch (CHR); and Dunedin (DUN)) followed by a three-digit patient number. The fourth digit indicates which of the five isolates from the patient is shown. Lower-case isolate names highlight two cases where patients were sampled twice, at different centres. Isolates belonging to overseas strains are from: Liverpool, UK (LES); Manchester, UK (MAN); Melbourne, Australia (pulsotype1.1 and pulsotype1.2) and Brisbane, Australia (pulsotype2). •, ○, ▴, ▵, ⋄: isolates obtained from five sibling pairs. ········: threshold genetic distance of 0.118 used for defining clusters of isolates with highly similar patterns. Grey bars show clusters present in only one New Zealand patient. Black bars show clusters present in several New Zealand patients. In more than two where a cluster was present in more than two New Zealand patients, the number of patients is shown to the right of the bar.
Transmission results in clusters of identical or very similar DNA types in different patients. To arrive at a meaningful threshold for identifying clusters, the genetic distance between two independent scores of the same pattern was determined in 50 instances, in two different DNA preparations. The average genetic distance was 0.094; the upper 95% confidence limit was 0.118. Therefore, 0.118 was used to define clusters and above this distance the present authors were confident of distinguishing different patterns.
In 67 patients, all isolates were identical or could be assigned to one cluster specific to this patient (grey boxes in fig. 1⇑) indicating that their isolates were derived from a single infecting strain. Isolates from the remaining 35 patients were too different to be placed into single patient-specific clusters (although often they were still more similar to each other than to isolates from any other patient). For the two patients who moved during the study and were sampled twice, GRE142/DUN242 and GRE144/WAI249 (lower case isolate labels in fig. 1⇑), isolates obtained at both centres fell into the same clusters, with one exception (gre144 3).
Some clusters contained isolates from two to nine different patients (black boxes in fig. 1⇑). Such clustering can result from transmission, clonal expansions predating and unrelated to transmission in the patient population under study, or simply because no typing method produces an infinite number of types 17. To estimate how much clustering is expected without transmission in the current patient population, the frequency of distance values <0.118 was calculated when only isolates obtained at different hospitals were compared (i.e. isolates lacking direct epidemiological connection; 1.9%; 336 out of 17,078 comparisons). Therefore without transmission, 1.9% of distance values resulting from all comparisons between isolates from different patients in figure 1⇑ should be <0.118. However, 2.2% (486 out of 21,366) of comparisons from patients in figure 1⇑ had distance values <0.118; 65 more than expected without transmission.
The present study next assessed if any of the clusters in figure 1⇑ involved a significantly higher proportion of patients from one centre, as expected if a cluster were resulting from transmission. This was the case only for the largest cluster (involving nine patients), isolated almost exclusively from patients attending the Greenlane CF Centre (seven out of 38 Greenlane patients had isolates that were part of this cluster, compared with two out of 66 patients from other clinics; Fisher’s exact test p = 0.012). Also, patients with isolates belonging to the cluster had more centre-related contact with each other than the remaining Greenlane patients (fig. 2⇓; p = 0.015; the sum of 21 pairwise physical distance category values for the seven patients was lower than the sum of 986 out of 1,000 sets of 21 values chosen randomly from a matrix of all remaining Greenlane patient pairwise physical distance category values), consistent with the hypothesis that transmission was healthcare-related.

Distribution of physical distance categories among Greenlane patients contributing to the largest cluster (▒) and the remaining Greenlane patients (░). I: siblings; II: patient pairs hospitalised in the same ward at overlapping times; III: patient pairs who attended outpatient clinics on the same day; IV: patient pairs where one attended an outpatient clinic at the same time the other was hospitalised; V: patient pairs who were hospitalised, or attended outpatient clinics, but never at the same time; VI: patient pairs who were not hospitalised and never attended clinics at the same time.
No significant (unpaired t-test) differences were found in several health status indicators (BMI, z-scores, FEV1 values, frequency of clinic attendance or days in hospital) between the nine patients carrying strains belonging to this shared cluster and all other study patients, or between the seven Greenlane patients carrying these strains and all other Greenlane patients. Also, the sex or age distribution of patients infected with cluster isolates did not differ significantly (Fisher’s exact and unpaired t-tests) from that of the remaining patients (data not shown).
Prevalence of potentially transmissible overseas strains in New Zealand
The introduction and spread of highly transmissible overseas strains is a potential threat to New Zealand patients. Therefore, representatives of four such strains were included in the current analysis to examine whether such strains might be spreading into New Zealand. New Zealand isolates clustering with three of the strains were found. Isolates with SalI types highly similar to the overseas strains also had PFGE types indistinguishable or closely related to those of the overseas strains (see online supplementary material; fig. 1⇑). The Manchester and pulsotype1 strains each clustered with isolates from a single New Zealand patient. The adult (GRE126) with an isolate indistinguishable from the Manchester strain had lived in London, UK, and it was there his initial P. aeruginosa infection was first detected. Another patient (CHR119) possessed isolates similar to Melbourne pulsotype1 isolates and had previously holidayed in Queensland, Australia, although without making contact with Australian CF clinics or patients. Brisbane pulsotype2 isolates formed a cluster with isolates from four New Zealand patients. Two patients (WEL101 and GRE144/WAI249) had previously lived in Brisbane where one first acquired P. aeruginosa before immigrating to New Zealand. Both had mixed freely with Australian CF patients while receiving treatment. The remaining two patients (GRE114, GRE185) had isolates resembling pulsotype2 and were treated in the same centre as, but were never in direct contact with, a patient previously exposed to pulsotype2 overseas (GRE144/WAI249). Thus at most three patients are likely to have acquired overseas strains in New Zealand.
Centre-related patient contact and distance between their isolates
Many of the centres in the present study had very small patient numbers, and in these transmission may only lead to very small clusters, and thus be difficult to detect by assessing clustering. Therefore, an alternative approach of searching for transmission was also used, by determining whether the genetic distance between patients’ isolates tends to decrease with increased patient contact.
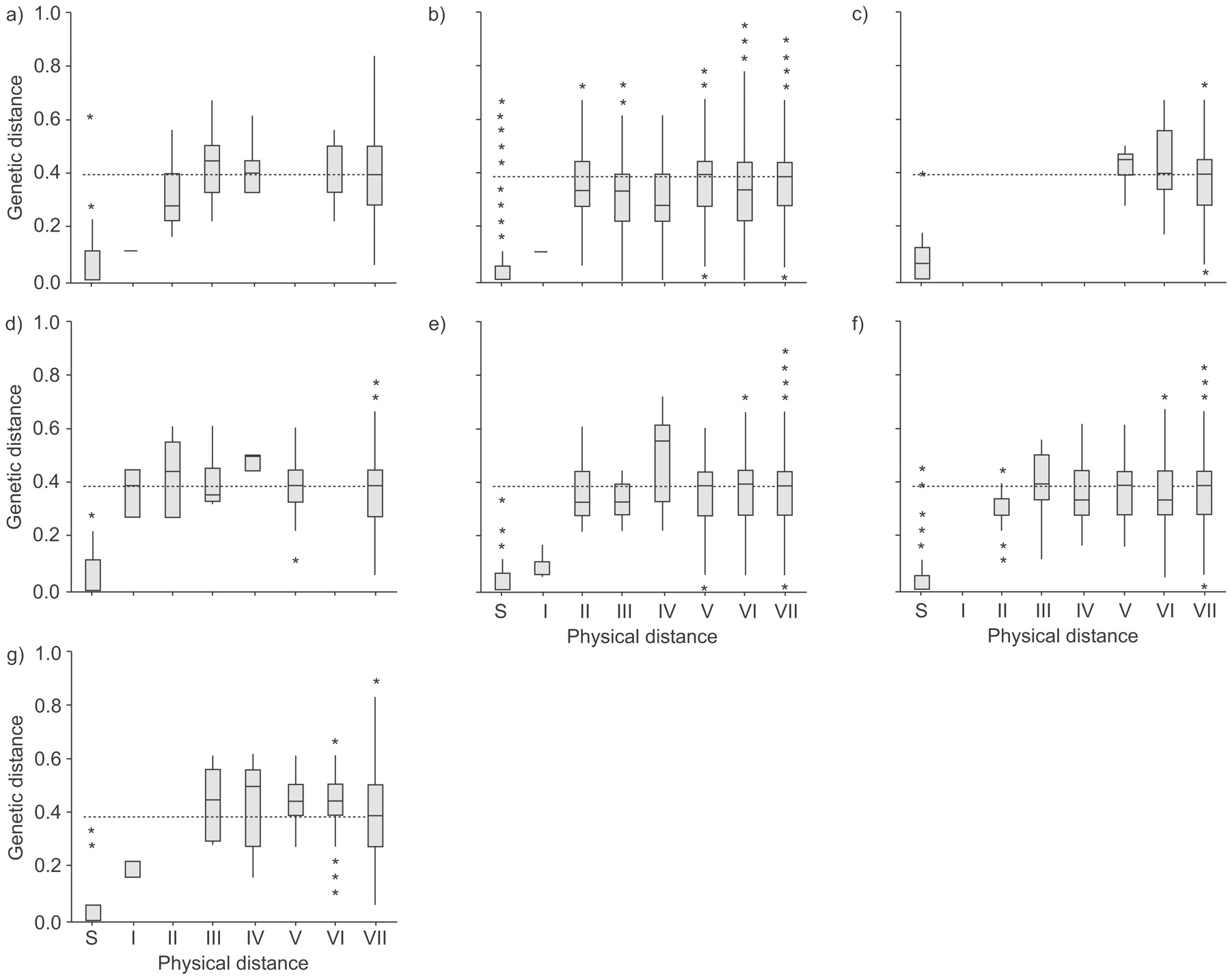
It was first determined if the closest-related counterparts of isolates from patients in a given clinic were isolates from other patients at the same clinic more often than expected by chance. This was not the case (see online supplementary material; table 1⇑). Next it was checked whether, within each clinic, the average genetic distance between patients’ isolates decreased as the degree of physical contact (and opportunity of transmission) increased (fig. 3⇓). For comparison in the analysis the distribution of genetic distances between isolates from the same patient and the distribution of genetic distances between isolates from a given centre and isolates from all other centres were included. Only isolates from different siblings were generally more similar to each other than isolates from pairs of patients treated in different centres, indicating that the multiple P. aeruginosa isolates in most sibling pairs were derivatives of a single strain. In contrast, the distribution of genetic distances between isolates from pairs of patients with various degrees of contact through treatment at the same centre was not significantly different from that between isolates from patient pairs treated at different clinics, although at Greenlane the median genetic distances, in all but one of these categories, were lower than those between isolates at Greenlane and those from patients at all other hospitals. The current study also failed to detect a dependence on the frequency of low genetic distance values on centre-related patient contact (see online supplementary material).

{kind=link}
{kind=link}
{kind=link}
Box and whisker plots of the distribution of genetic distances between isolate pairs from patients with different degrees of physical contact in New Zealand cystic fibrosis clinics: a) Starship (Auckland); b) Greenlane (Auckland); c) Waikato (Hamilton); d) Palmerston North; e) Wellington; f) Christchurch; and g) Dunedin. S: pairs of isolates from the same patient; I: siblings; II: patient pairs hospitalised in the same ward at overlapping times; III: patient pairs who attended outpatient clinics on the same day; IV: patient pairs where one attended an outpatient clinic at the same time the other was hospitalised; V: patient pairs who were hospitalised, or attended outpatient clinics, but never at the same time; VI: patient pairs who were not hospitalised and never attended clinics at the same time; VII: pairs of isolates from pairs of patients treated in different hospitals, i.e. the genetic distances in category VII are those between isolates obtained in the hospital the figure refers to and isolates in all other hospitals. ········: median of genetic distances in category VII.
Lastly, it was determined whether the four patients who first acquired P. aeruginosa during the course of the present study (WEL110, CHR235, WELL243 and PAL257) harboured isolates closely related to those from other CF patients at the same clinic. In each case the isolates in the current sample closest related to theirs were not from the same centre.
DISCUSSION
Transmission of P. aeruginosa between New Zealand CF patients appears infrequent. Isolates from patient pairs with frequent treatment-related contact are generally not more closely related than those from patients attending different centres. This also indicates that, with the possible exception of siblings who often share similar strains, social contact generally did not lead to significant transmission: otherwise, isolates from patients treated in the same centre should be more closely related than isolates from patients treated in different centres hundreds of kilometres apart.
The only evidence for healthcare-related transmission is a cluster of isolates in seven out of 38 patients at Greenlane. The cluster is overrepresented in Greenlane where patients with isolates belonging to the cluster were in closer contact with one another than other Greenlane patients. Also the cluster’s size (97 distance values <0.118 among cluster isolates from Greenlane) roughly matches the excess of distance values <0.118 in the present patient population indicative of transmission.
Evidence for transmission is also consistent with the current authors’ earlier findings 23 of reduced genetic diversity of isolates from CF patients compared with isolates from other Greenlane patients, but together the two studies also indicate that transmission is uncommon at Greenlane. The cluster’s prevalence has not changed significantly in the 8 yrs since the earlier study, when cluster isolates were present in three out of 20 CF patients 23, and had not increased among five patients participating in both studies where one of these patients (GRE 107) had cluster isolates on both occasions. Furthermore, three out of the remaining four patients (GRE102, 105, 123 and 145) also retained their original strains. Likewise the pulsotype2 strain, capable of spreading overseas, had not done so in Greenlane to a readily demonstrable degree. Two patients may have acquired the strain while at Greenlane. However, no direct epidemiological connection was identified, and the main Greenlane cluster can account for all transmission-related clustering in the present sample, arguing against transmission as a cause of the pulsotype2 cluster. Thus, because typing methods do not give an unlimited number of patterns and sample only a small part of the genome 17, 23, the pulsotype2 isolates from the two patients may only be similar to, but not derived from, the overseas pulsotype2 strain.
Current infection control measures thus appear to protect patients from transmission in New Zealand clinics, except for the cohort presently attending Greenlane where a recent report also suggested cross-infection by Burkholderia multivorans may have taken place 29. When interpreting these data, the small size of New Zealand CF clinics must be considered. Patients in smaller centres usually have less contact with one another 30 and thus less opportunity to transmit strains. Certainly, the clinic where the evidence was found for transmission was by far the largest in the current study, with substantially more patient contact compared with other centres. The present results raise the possibility that the existing body of research, based largely on findings in large CF clinics, may overestimate the risk of cross-infection among the many CF patients who are still treated in smaller centres. Furthermore, smaller centres also make it harder to detect transmission by visual inspection of dendrograms. However, the analysis in figure 3⇑ and the current analysis based on the expected frequency of distance values <0.118 in the entire sample without epidemiological contact should have revealed any transmission occurring in other centres. It could be argued that the latter analysis may have underestimated transmission among the present study patients, since its calculations are based on the assumption that patients treated in different centres lack any epidemiological connection. This is not entirely accurate, as patients do move between clinics. Two such movements were recorded during the present study and additional movement will have occurred before the investigation. However, the error in the current estimated frequency of distance values <0.118 between unconnected isolates is probably small. It had been determined earlier 23 that the discriminatory power of the current method (probability that two unrelated isolates can be discriminated), was 0.99, using isolates from unrelated non-CF patients where unexpected epidemiological relationships are very unlikely. In the current study, 1.9% of pair-wise comparisons between representative isolates from patients treated in different centres were not reliably distinguishable from one another (genetic distance <0.118), equivalent to a discriminatory power of 0.98. This means that isolates from different centres in the present study were approximately as epidemiologically unconnected as isolates from epidemiologically unrelated non-CF patients.
This new estimate of discriminatory power, the finding that SalI patterns are stable over 7–8 yrs and observing isolates that formed clusters with the present method were also indistinguishable by pulse-field gel electrophoresis, all confirm SalI typing as an attractive alternative to pulse-field gel electrophoresis, in particular if cost is considered as well. The current study indicates that surveillance of the total New Zealand cystic fibrosis population would cost ∼US$8,000 per year.
Support statement
The New Zealand Child Health Research Foundation (Auckland, New Zealand) provided financial support for the present study.
Statement of interest
None declared.
Acknowledgments
The present authors would like to thank A. Farrell, D. Graham, P. Jackson, M. O’Carroll, M. Tweed, A. Watson, M. Wilsher, M. Hoggard, V. Isles, J. Tate, L. Thrift, K. Brassett and A. Williamson for assistance with recruitment, sample and data collection; M. Bilkey, C. Brehmer, J. DeLores, H. Maguire, L. McKnight, J. Parker, C. Pickett, R. Podmore, K. Stockman and A. Van Der Linden for identification of isolates; U. von Mulert for database design; A. Grinberg and R. Pattison for assistance with PFGE; A. Morris for comments on the manuscript; and A. Palamountain for programming.
Footnotes
-
This article has supplementary material accessible from www.erj.ersjournals.com
- Received July 1, 2008.
- Accepted August 1, 2008.
- © ERS Journals Ltd
References










