





Abstract
We need markers in CF that identify those susceptible to a severe pulmonary course. We have already shown that LCI at 4y predicts lung function at 6-10y(Aurora AJRCCM 2011).
Methods: 27 clinically diagnosed CF children had LCI & spirometry recorded at preschool & adolescence.
Results: Mean age at pre-school test was 4.3y(range 3.2-5.7y) and adolescence 15.0y(12.6-17.9y). Preschool LCI was abnormal in 15/27(56)% and FEV0.75 in 6/25(24%). By adolescence 23(85%) had abnormal LCI and 9(33%) abnormal FEV1.
| Abnormal adolescent LCI | Normal adolescent LCI | Abnormal adolescent FEV1 | Normal adolescent FEV1 | |
| Normal preschool LCI | 14 | 1 | 6 | 9 |
| Abnormal preschool LCI | 9 | 3 | 3 | 9 |
| Normal preschool FEV0.75 | 5 | 1 | 4 | 2 |
| Abnormal preschool FEV0.75 | 16 | 3 | 3 | 16 |
Abnormal test defined by ≥+1.96 z-scores(Lum 2013) for LCI and ≤-1.96 z-scores for forced expired volumes(Quanjer 2012).
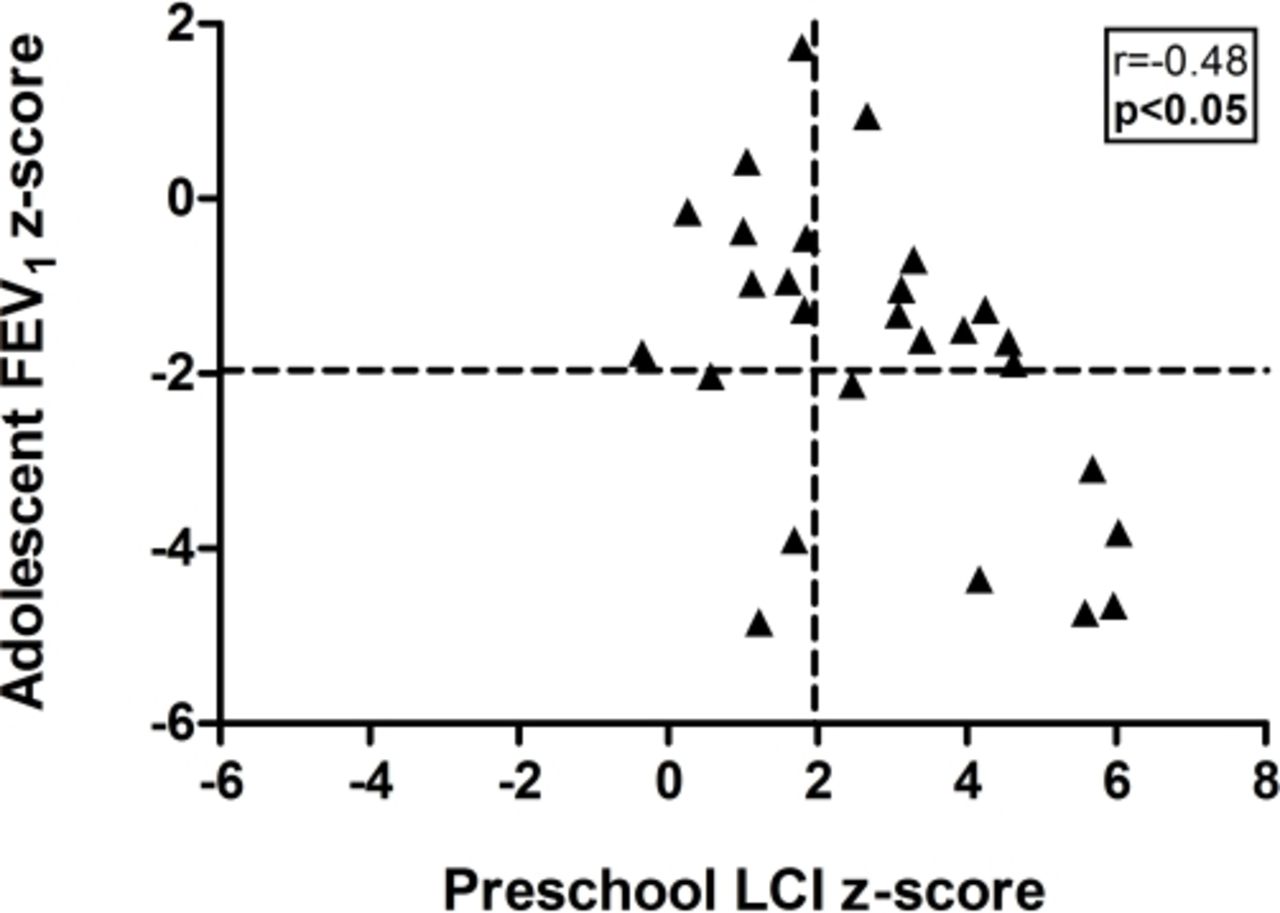
If a true positive is both abnormal preschool & adolescent test:then positive predictive value(95% CI) of preschool LCI for adolescent FEV1 was 40%(20,64%) & negative predictive value(NPV) 75%(47,91%). Preschool LCI correlated with adolescent LCI(r=0.59,p<0.01) & FEV1(r=-0.48,p<0.05). There was no correlation between preschool & adolescent spirometry. Most children with abnormal spirometry in adolescence had abnormal preschool LCI, but the converse did not apply(figure).
{kind=link}
Conclusion: NPV of preschool LCI for adolescent FEV1 is good and may identify children with milder disease.
- Copyright ©ERS 2015









