





Abstract
Diffuse alveolar haemorrhage (DAH) is a feature of several immune and nonimmune disorders. Reported prognosis is poor, with in-hospital mortality ranging from 20% to 100%. Early identification of prognostic factors may be useful in the initiation of appropriate treatment.
We retrospectively analysed the charts of all patients referred to a university hospital for DAH between 1980 and 2008. Variables associated with in-hospital and long-term mortality were determined using a logistic regression model and the Kaplan–Meier method, respectively. Immunosuppressed patients were excluded.
Overall, 97 patients were included in the study. In-hospital mortality was 24.7%. Factors associated with in-hospital mortality were shock (OR 77.5, 95% CI 8.9–677.2), glomerular filtration rate <60 mL·min−1 (OR 11.2, 95% CI 1.8–68.4) and plasmatic lactate dehydrogenase level more than twice the normal value (OR 12.1, 95% CI 1.7–84.3). Mortality among discharged patients was 16.4% with a median follow-up duration of 34 months. Factors associated with increased long-term mortality in univariate analysis were age over 60 yrs (p = 0.026), cardiovascular comorbidity (p = 0.027) and end-stage renal failure with dependence on haemodialysis (p = 0.026).
Patients with immune and nonimmune DAH had similar outcomes. Early outcome depended on nonpulmonary organ failures. Conversely, late outcome was related to age, cardiac comorbidities and the need for haemodialysis.
Diffuse alveolar haemorrhage (DAH) is a feature of several immune and nonimmune disorders. The fundamental process common to each of the DAH syndromes is diffuse bleeding into the acinar portion of the lung. It typically presents with haemoptysis, anaemia and pulmonary infiltrates on chest radiograph. Failure to diagnose and treat DAH syndromes in their early stages may lead to acute respiratory failure and death. Reported prognosis is poor, with in-hospital mortality ranging from 20% to 100% 1–3. Delay in initiating treatment may lead to chronic renal failure when DAH is the early manifestation of a systemic disease 4, 5.
Early identification of factors associated with a poor outcome may be useful in selecting the patients at highest risk to initiate appropriate treatment. To our knowledge, no publications currently address this question. Most published series are limited and instead focus on immune causes of DAH 4–6. Long-term outcomes and factors associated with mortality in patients with DAH after discharge have not been studied. This information may be important in decision making.
Therefore, we conducted a retrospective study in a large cohort of consecutive patients hospitalised for symptomatic DAH over a 29-yr period. Immunocompetent individuals presenting with a DAH of immune or nonimmune cause were included. We sought to identify early predictors of in-hospital mortality available within the first 24 h following hospital admission and factors associated with long-term mortality in discharged patients.
METHODS
Study design
A retrospective cohort study was performed in the intensive care unit (ICU) and chest department of an 800-bed tertiary hospital in France (Hôpital Tenon, Assistance Publique-Hôpitaux de Paris, Paris, France). This observational, noninterventional analysis of medical records was approved by the institutional review board of the French Learned Society for Respiratory Medicine, Société de Pneumologie de Langue Française (Paris, France).
Subjects, data collection and definitions
The medical records of consecutive patients admitted between January 1980 and May 2008 were reviewed. For patients admitted more than once, only the first admission was considered. All adult patients with symptomatic DAH were eligible. The definition of symptomatic DAH was based on the following criteria. First, the clinical and radiological presentation was compatible with the diagnosis of DAH (haemoptysis, new pulmonary infiltrates and anaemia) 4. Secondly, the bronchoalveolar lavage (BAL) fluid was macroscopically bloody. Alternatively, haemorrhagic and siderophagic alveolitis were evidenced on BAL cytology 7, transbronchial lung biopsy or surgical lung biopsy. Diagnosis of DAH was definite when all the above criteria were met.
Patients with immunocompromised status (HIV infection, solid or haematological malignancies, bone marrow or solid organ transplantation, immunosuppressive drug therapy, cytotoxic chemotherapy or radiotherapy, steroids at a daily dose >20 mg of prednisone-equivalent for >2 months) were excluded. Patients with haemorrhage of bronchial origin and patients receiving haemodialysis for chronic renal failure were also excluded.
Variables available during the first 24 h of hospitalisation included demographic data (age and sex), body mass index, alcohol use (defined by the World Health Organization as >40 g·day−1 for males and >20 g·day−1 for females), current or former tobacco exposure, past medical history (especially respiratory and cardiovascular diseases) and ongoing anticoagulant and/or antiaggregant treatment. Clinical variables and laboratory data related to the pulmonary disorder at admission included the following: time elapsed between the first symptoms and hospital admission, respiratory rate, haemoptysis, accessory muscles use, presence of crackles, need for invasive mechanical ventilation, arterial blood gas analysis with arterial oxygen tension (Pa,O2)/inspiratory oxygen fraction (FI,O2) ratio (non-mechanically ventilated patients had arterial blood gases measured while breathing room air), chest radiograph and BAL characteristics (total cell count, formula and percentage of siderophages on Perls staining and microbiology).
Nonpulmonary clinical variables were also recorded, including weight loss >5% of baseline body weight in the last 3 months, body temperature, blood pressure, heart rate, presence of shock, extrapulmonary symptoms (skin, bone and joint, gastro-intestinal, neurological, nose–ear–throat or ocular), and haematuria or proteinuria on urinalysis reagent strip. Shock was defined by a mean systemic blood pressure <60 mmHg after 20–30 mL·kg−1 starch or 40–60 mL·kg−1 saline, or a pulmonary capillary wedge pressure between 12 and 20 mmHg and the need for dopamine >5 μg·kg−1 per min or dobutamine, norepinephrine or epinephrine, whatever the infusion rate, to maintain mean blood pressure >60 mmHg 8, 9. Laboratory data included glomerular filtration rate calculated with the Cockroft formula, haemoglobin, blood leukocyte count, platelet count, thromboplastin time, partial thromboplastin time and lactate dehydrogenase (LDH).
The time elapsed between hospital admission and the first dose of steroids, if administered, was recorded. The severity of DAH was assessed from generic scores of organ dysfunction including the Logistic Organ Dysfunction (LOD) score 10 and the Simplified Acute Physiology Score (SAPS) II 11. The need for chronic haemodialysis and pulmonary disability after discharge were recorded.
The aetiologic diagnoses of DAH were specifically defined. The American College of Rheumatology criteria were used for defining a necrotising vasculitis. A histological proof of necrotising vasculitis was required 12–15. The American Rheumatism Association criteria were used for defining a connective tissue disease 16, 17. The anti-glomerular basement membrane antibody disease was diagnosed when the serologic test for anti-glomerular basement membrane antibodies was positive. Alternative diagnosis was made on the presence of a linear immunofluorescent glomerular immunoglobulin deposit 18. Clinical and radiological features suggestive of DAH related to an increased pulmonary capillary pressure 19 were an increased left atrial pressure (detected by Doppler echocardiography or right heart catheterisation, which were performed in 82 and 10 patients, respectively; see figure 1⇓ in the online supplementary material), and respiratory improvement after forced saline diuresis 20, 21. The diagnosis of a barotraumatic stress capillary failure due to a negative pulmonary pressure (tracheal extubation or scuba diving) was made in a suggestive context 22, 23. For cancer, the presence of histological evidence was used in the diagnosis. For infection, positive microbiological or serological tests allowed for diagnosis. Clotting disorders were diagnosed by a platelet count <150,000 cells·mL−1, a patient-to-control subject ratio of activated partial thromboplastin time >1.5, or a thromboplastin time <60%. The diagnosis of toxin-induced or drug-induced disease was established when there was a compatible chronology after exposure to a known pneumotoxic substance. This diagnosis required the exclusion of all the other causes of DAH 24. Idiopathic DAH was defined when a thorough search for the above-mentioned causes remained negative.

Flow chart of patients hospitalised between 1980 and 2008 for diffuse alveolar haemorrhage (DAH). ICU: intensive care unit. #: missing data (n = 10), haemorrhage of bronchial origin (n = 43) or discovery of an immunocompromised status during hospitalisation (n = 1).
Data presentation and statistical analysis
Standard descriptive statistics were computed. Continuous variables were reported as median (interquartile range), unless otherwise stated. The Shapiro–Wilk normality test was performed. We then drove two different models to assess the factors associated with in-hospital and long-term mortality, because we considered that each one of them addressed specific clinical issues. Univariate and multivariate logistic regressions were used to identify factors associated with in-hospital mortality. Cut-off values were then defined according either to their median (<60 mL·min−1 for glomerular filtration rate) or to a clinically relevant threshold (>20 pack-yrs for tobacco use, <10 g·dL−1 for haemoglobin and >2 upper normal value for LDH). A time variable referring to the year of hospitalisation (from 1 for 1980 to 29 for 2008) was used to assess the dependency of the outcome upon time, given the length of the study period. Variables yielding p-values <0.05 by univariate analysis and considered clinically relevant were entered into a forward multivariate logistic regression analysis. Odds ratios and their 95% confidence intervals were computed. Colinearity and interactions were tested. We chose to enter a maximum of three variables in the final multivariate model in order to avoid overfitting 25. A base model including the main organ failures (shock and respiratory and renal failures) was created. These variables have been chosen because they have been previously shown to strongly influence the outcome of patients with acute respiratory distress syndrome 26. The other covariates were entered in the model with a critical removal p-value of 0.1. Effects on covariate coefficients were also considered. The SAPS II score and LOD score were not entered in the multivariate analysis because they encompassed other study variables (age as well as other variables used to define organ failures) 10, 11. Long-term outcome was studied for patients discharged from the hospital. Factors associated with long-term mortality were identified by the Kaplan–Meier method with the log-rank test. No further multivariate analysis was performed because the statistical power was considered too low. Two-tailed p-values <0.05 were considered statistically significant. Analyses were carried out using Statview statistical software (SAS Institute Inc., Calasabas, CA, USA).
RESULTS
Patient characteristics
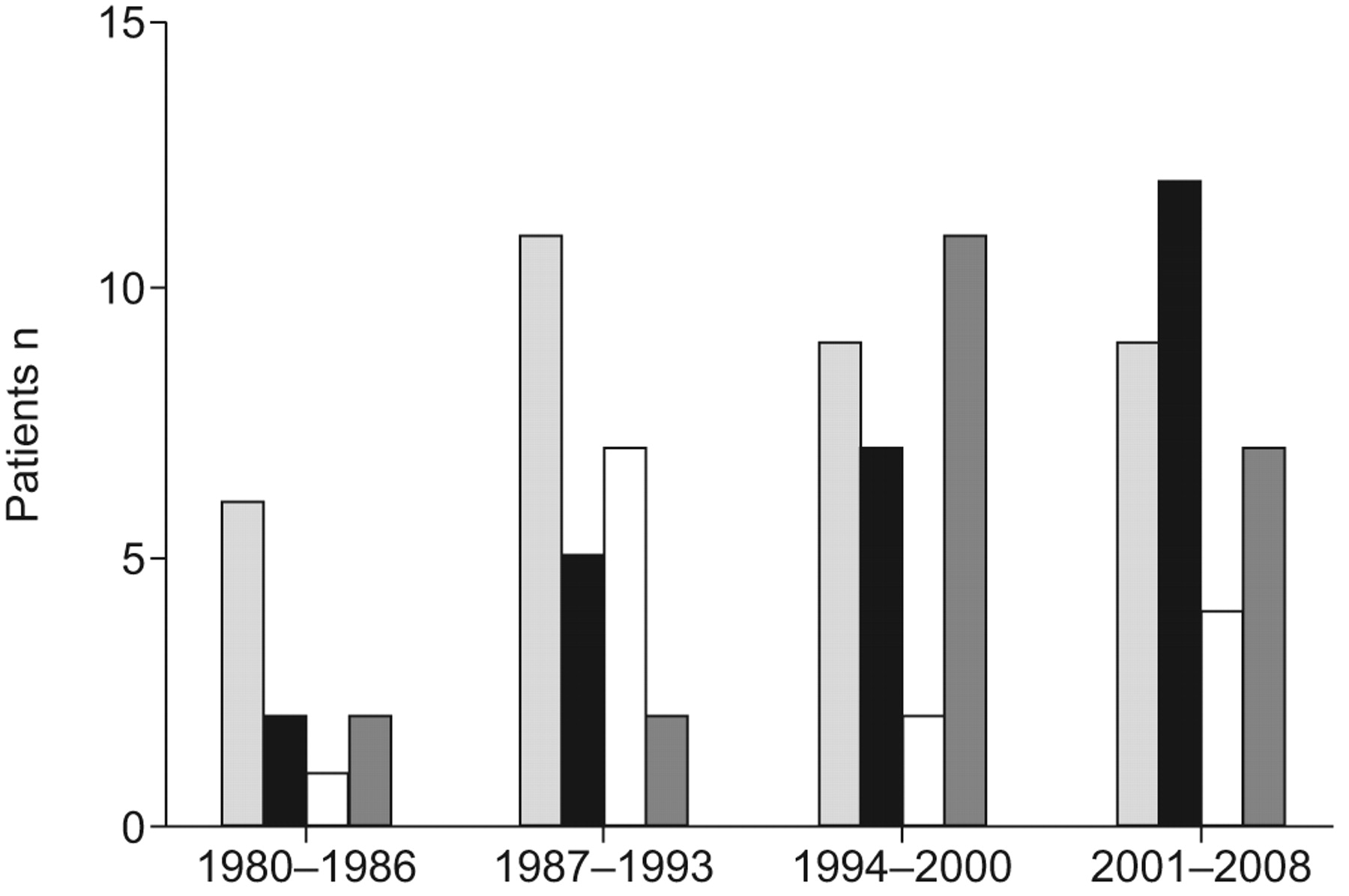
Overall, 151 patients suspected of DAH were eligible, 54 of whom were not included due to missing data (n = 10), haemorrhage of bronchial origin (n = 43) or evidence of an immunocompromised status during hospitalisation (n = 1) (fig. 1⇑). Of the remaining 97 patients included in the cohort study, 73 were hospitalised in the ICU and 24 in the chest unit. The main causes of DAH are listed in table 1⇓. One-third of the DAH syndromes were immune. The distribution of the causes of DAH over four time periods (1980–1986, 1987–1993, 1994–2000 and 2001–2008) is depicted in figure 2⇓. The baseline characteristics of the 97 patients at admission are shown in table 2⇓.

Causes of diffuse alveolar haemorrhage (DAH) for patients hospitalised over four time periods. ░: immune DAH; ▪: increased pulmonary capillary pressure; □: idiopathic; ▒: miscellaneous.
Aetiology of diffuse alveolar haemorrhage(DAH) syndromes
Characteristics and initial presentation of the 97 patients
The median length of stay was 12 (6–20) days, averaging 14 (10–22) days for ICU patients and 10 (7–15) days for conventional chest ward patients. Intravenous steroids were administered to 39 patients after a median of 2 (1–5) days after hospital admission. In-hospital mortality rate was 24.7% (24 out of 97) and did not vary significantly over time (five out of 11, 45.4%, during 1980–1986; six out of 25, 24%, during 1987–1993; five out of 29, 17.2%, during 1994–2000; and eight out of 32, 25.0%, during 2001–2008; p = 0.58). Accordingly, there was no relationship between the year of hospitalisation and hospital mortality in univariate analysis (OR 0.97, 95% CI 0.91–1.03; p = 0.27). The median follow-up duration was 34 (9–84) months for discharged patients, with a mortality rate of 16.4% (n = 12). Overall mortality rate was 37.1% (36 out of 97).
Figure 3a⇓ shows the Kaplan–Meier curve of survival probability over time for all patients. Finally, Kaplan–Meier curves of patients having a DAH related to increased pulmonary capillary pressure or not (fig. 3b⇓) or related to an immune cause or not (fig. 3c⇓) were drawn for the whole study population. There was a higher overall mortality in patients with DAH related to increased pulmonary capillary pressure, as compared with patients with DAH not related to increased pulmonary capillary pressure (14 out of 26, 54% versus 22 out of 71, 31%, respectively; p = 0.019 by the log-rank test). In contrast, patients with immune DAH did not have a different overall prognosis, as compared with patients with non-immune DAH (12 out of 35, 34% versus 24 out of 62, 39%; p = 0.738 by the log-rank test).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curves of the probability of survival during the median follow-up period. ······: separation between in-hospital mortality and mortality in discharged patients. a) Kaplan–Meier curve showing the probability of survival for all patients. b) Kaplan–Meier curve showing the overall probability of survival for patients with (–––––) or without (– – –) diffuse alveolar haemorrhage (DAH) related to increased pulmonary capillary pressure (IPCP); p = 0.019 (log-rank test). DAH not related to IPCP includes immune and idiopathic DAH and DAH of miscellaneous causes. c) Kaplan–Meier curve showing the overall probability of survival for patients with immune (–––––) or nonimmune (– – –) related DAH; p = 0.735 (log-rank test). Nonimmune DAH include DAH related to IPCP, idiopathic DAH and DAH of miscellaneous causes.
Prognostic factors of hospital mortality
24 patients (24.7%) died in hospital, 22 of whom were hospitalised in the ICU. Age >60 yrs, previous cardiovascular disease, tobacco history >20 pack-yrs, need for invasive mechanical ventilation, shock, LDH greater than twice the normal value and glomerular filtration rate <60 mL·min−1 yielded a p-value <0.05 in univariate analysis and were considered for the multivariate analysis (table 3⇓). Three factors were independently associated with in-hospital mortality in the multivariate analysis, including shock (OR 77.6, 95% CI 8.9–677.2), glomerular filtration rate <60 mL·min−1 (OR 11.2, 95% CI 1.8–68.4) and plasmatic LDH greater than twice the normal value (OR 12.1, 95% CI 1.7–84.3). The Pearson goodness of fit test yielded a p-value >0.05 (p = 0.95), meaning that the calibration of the model was good. The r2 yielded by the model was 0.52.
Univariate and multivariate analysis of variables associated with in-hospital mortality available within the 24 h following admission
Prognostic factors of long-term outcome
The mortality rate of the 73 discharged patients was 16.4% (12 out of 73) during the follow-up period. Age >60 yrs (p = 0.026), a previous cardiovascular disease (p = 0.027) and a persistent renal failure requiring chronic haemodialysis (p = 0.026) were associated with long-term mortality in the univariate analysis performed with the Kaplan–Meier method. Figure 2⇑ of the online supplement shows the Kaplan–Meier curves of survival representing a patient's probability of survival over time based on the presence of a previous cardiovascular disease (p = 0.027).
DISCUSSION
Our study reports the outcome of 97 patients hospitalised in a tertiary hospital for an initial episode of DAH. DAH may result from a broad spectrum of diseases of different pathophysiological mechanisms. However, diagnosis of the underlying condition can be challenging and may not be known within the first hours following hospital admission. We therefore aimed to identify available factors on admission that were associated with a poor prognosis. As a result, the study population reflects the large and heterogeneous spectrum of the diseases that may be encompassed in the setting of DAH. The overall mortality rate was 37.1%, combining the 24.7% rate of in-hospital mortality and the further post-discharge mortality rate of 16.4%. Different prognostic factors were related to the in-hospital and long-term mortality. The first group of factors included LDH level, shock and renal failure. The second group of factors included age >60 yrs, cardiovascular disease and the need for chronic haemodialysis.
DAH is a rare and severe syndrome with a reported in-hospital mortality of 20–100% 1–3. Previous series included limited samples of patients with immune DAH and reported that the main causes of death were infections and renal failure 4, 5, 27, 28. Although DAH of immune causes are usually deemed to have a poorer prognosis than DAH of nonimmune causes 4, there is to our knowledge no study assessing the determinants of outcome in a cohort including DAH of immune and nonimmune causes. In our series, the in-hospital mortality rate was 24.7%, emphasising the poor prognosis for patients experiencing an initial episode of DAH, even in a nonselected population of patients. These results highlight the need for a tool to quickly identify patients who would benefit from aggressive treatment and intensive monitoring.
Three factors available during the first 24 h of hospitalisation were independently associated with in-hospital mortality. We did not enter the SAPS II and the LOD scores into our statistical model in an attempt to identify the specific organ failures related to a poor prognosis. Accordingly, the in-hospital mortality was predicted by extrapulmonary organ failures (shock and renal failure), underlining the fact that most patients were affected by general diseases (immune disorders and cardiovascular diseases) that led to cardiac and renal failure 18, 29–31. Half (nine out of 17; 53%) of the patients with shock had a DAH related to increased pulmonary capillary pressure. Among those nine patients, eight had a pre-existing cardiovascular disease. We thus hypothesise that those patients had a cardiogenic shock associated with DAH due to increased pulmonary capillary pressure, both complicating severe/end-stage left heart failure. Eight other patients, among whom only one survived, had shock: three had septic shock (three patients with Panton–Valentine producing Staphylococcus aureus) and five had a multiple organ failure syndrome of an unclear mechanism (two patients with idiopathic DAH, two patients with immune DAH and one patient with clotting disorder). However, the underlying cause of organ failure (immune versus nonimmune) was not related to outcome, as the overall mortality did not differ between patients with or without an immune cause of DAH. Surprisingly, the variables related to respiratory failure (need for invasive mechanical ventilation or Pa,O2/FI,O2 <200 mmHg at admission) did not appear to predict mortality in our model. This may be explained by interdependence with the variable shock. Shock was indeed strongly related to hospital mortality (p<0.0001 for each of the respiratory failure variables). Conversely, the fact that increased LDH level at admission was a risk factor for hospital mortality in our series probably reflected the prognostic impact of pulmonary injury. Previous studies have demonstrated that increased LDH level in patients with pulmonary pneumocystosis or acute respiratory distress syndrome is a prognostic factor 32, 33. However, increase in LDH level can be the result of various conditions which makes its interpretation speculative 34.
12 of the 73 patients discharged from our hospital died during the follow-up period. This resulted in a low statistical power. Therefore, no multivariate analysis was performed on the factors associated with long-term outcome with the Kaplan–Meier method. Age >60 yrs was associated with mortality in discharged patients. This finding was in agreement with the study of Thibault et al. 35, who found that age had a greater effect on long-term mortality in a large nonselected population of patients admitted to the ICU. Dependence on haemodialysis was also a risk factor for long-term mortality. This was a result of pulmonary–renal syndrome that led to end-stage renal failure 18, 28. Previous studies showed that renal failure is an independent predictor of poor outcome in anti-glomerular basement membrane antibody disease 18, connective tissue disease 36 and vasculitis 37. This suggests that a subgroup of patients suffering from immune causes of DAH leading to end-stage renal failure might be at higher risk of death, although the limited statistical power of our study did not allow us to draw such an inference. Interestingly, patients with a pre-existing cardiovascular disease had an increased risk of death after hospital discharge. This finding suggests that DAH related to increased pulmonary capillary pressure may be associated with a worse prognosis than DAH related to other causes. Most of our patients with DAH related to increased pulmonary capillary pressure (19 out of 26; 73.1%) had a previously known cardiovascular disease, suggesting that DAH was the end-stage manifestation of a chronic heart disease that resulted in death in 12 patients. However, DAH was the first manifestation of a heart disease in seven patients (mitral stenosis, n = 3; left heart systolic dysfunction, n = 3; and diastolic dysfunction, n = 1), which led to death in two. In our series, patients with DAH related to increased pulmonary capillary pressure had a 53.8% overall mortality rate. In comparison, there was a 31.0% overall mortality rate in others (p = 0.019). Previously published data has reported a 33% 1-yr mortality rate in patients hospitalised for cardiogenic pulmonary oedema 29. Our findings support this study because DAH related to increased pulmonary capillary pressure was associated with a poor prognosis. For patients hospitalised before the era of echocardiography, the pulmonary artery occlusion pressure was measured (n = 10). We acknowledge, however, that among patients with increased pulmonary capillary pressure, some of those hospitalised in the 1980s might have been misclassified given the difficulty of assessing left ventricle diastolic function. It is thus likely that some of the patients classified as systolic dysfunction of the left ventricle had an associated diastolic dysfunction. However, all the patients classified as DAH due to increased pulmonary capillary pressure (n = 26) had a patent DAH, as opposed to a usual cardiogenic alveolar oedema: BAL fluid was macroscopically bloody in 10 patients, pink in 10 and normal in six, for whom the percentage of alveolar siderophages was always >70%. The discrimination of these patients from the others was therefore challenging on hospital admission. We thus wished to include them in this series, although the mechanisms involved in these DAH are mainly related to an increase in hydrostatic pressures and not to a primary lesion of the alveolocapillary barrier, as in DAH of other causes. This subgroup of DAH seems to exhibit a worse outcome than the others and might, therefore, require a more aggressive management. Anticoagulant or antiaggregant therapy was not associated with increased in-hospital or long-term mortality in this study (p = 0.11 and p = 0.43, respectively). However, these treatments may exacerbate alveolar haemorrhage. In particular, this may have occurred in patients with DAH related to left heart failure. These patients frequently receive such treatments. Among the 26 patients with DAH related to increased pulmonary capillary pressure, those who received anticoagulant or antiaggregant therapy trended towards a higher in-hospital mortality rate than the others (11 out of 18, 61.1% versus none out of eight, 0.0%; p = 0.076). This finding should be interpreted cautiously, as it might reflect the severity of the underlying heart disease. However, DAH has been frequently reported in patients receiving thrombolytic therapy in the setting of acute myocardial infarction. Alveolar bleeding may be facilitated by increased systolic pulmonary arterial pressure up to 65 mmHg, in accordance with animal models 38, 39. In rabbits, an artificial rise in capillary pressure leads to breaks in the alveolocapillary barrier 40, 41. Such intermediate forms of pulmonary oedema, which combine increased permeability and hydrostatic pressure, have been described in patients with heart failure 42. Whether clotting disorders may exacerbate the alveolar bleeding in the setting of capillary stress failure remains uncertain. However, withdrawing anticoagulant and/or antiaggregant therapy, at least temporarily, in patients with DAH due to increased pulmonary capillary pressure might be a suitable intervention which would need to be tested in further studies.
This study has several limitations. First, it is a retrospective study which covers a long period during which diagnosis tools, treatments and global quality of care might have varied; secondly, it is a monocentric study, which limits the potential of extrapolation of the conclusions drawn. However, the facts that 1) immunocompromised hosts were excluded; 2) the patients were all diagnosed and treated in the same institution; and 3) only basic clinical and radiological characteristics and biological tests were used to determine prognosis limit the risk of heterogeneity of practices during time. Main changes in practices over the 29 yrs of this study included 1) the increased use of Doppler echocardiography over time (from ∼50% in the 1980s to up to ∼100% during the last 14 yrs of the study) and the parallel decrease in the use of right heart catheterisation (see figure 1⇑ of the online supplement), and 2) the changes in the ventilatory management of patients with acute respiratory distress syndrome (i.e. tidal volume reduction) are likely to have improved their prognosis. Finally, the fact that a time variable was not associated with in-hospital mortality in univariate analysis does not preclude the possibility of an impact of time on outcome since the study was neither designed nor powered to test this hypothesis.
In summary, we reported a large series of immunocompetent patients hospitalised for initial episodes of DAH (immune and nonimmune). Predictors of in-hospital mortality available during the first 24 h following admission included shock, renal failure and increased LDH level, whatever the underlying cause of DAH. In contrast, long-term mortality was determined by age, cardiac comorbidities and dependence on haemodialysis. Further studies are needed to clarify the role of anticoagulant and antiaggregant therapy on the initial severity and outcome of DAH patients. This therapy may have a significant impact on those with left heart failure.
Statement of interest
None declared.
Footnotes
-
This article has supplementary material available from www.erj.ersjournals.com
- Received May 8, 2009.
- Accepted September 13, 2009.
- © ERS
References










