





Abstract
Significant survival heterogeneity exists in cystic fibrosis. Our aim was to determine whether residual function of the cystic fibrosis transmembrane conductance regulator (CFTR) is present in long-term survivors with severe mutations.
Nasal potential difference (PD) and sweat chloride were measured in 34 long-term survivors (aged ≥40 yrs) and compared with young patients (18–23 yrs) with severe (n = 30) and mild (n = 31) lung disease.
Baseline PD was not significantly different across the three groups (long-term survivors, -42.8 (range -71.0– -20.5) mV; young/mild, -40.5 (-58.8– -19.5) mV; young/severe,-46.3 (-74.0– -20.0) mV). Response to amiloride (ΔAmil) was significantly different across the three groups (p = 0.01); long-term survivors had values (27.8 (range 8.5–46) mV) which were not different to either young group, but the young/severe group had significantly higher values (29.5 (11–47) mV) than those in the young/mild group (22.0 (7–39) mV; p<0.01). Baseline PD and ΔAmil were associated with forced expiratory volume in 1 s (FEV1) (co-efficient (95% CI) -0.13 (-0.23– -0.03); p = 0.009 and -0.12 (-0.20– -0.04); p = 0.003, respectively). Sweat chloride was lowest (p <0.05) in the young/severe group (93.5 (74–111) mmol·L−1 versus 98.8 (76.5–116.0) mmol·L−1; long-term survivors; and 99.5 (80.0–113.5) mmol·L−1; young/mild).
Δ Amil is associated with FEV1 but our findings indicate that long-term survival cannot be explained by residual CFTR function when measurements are taken in later life.
Cystic fibrosis (CF) is an autosomal recessive condition caused by mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene and characterised by abnormal airway ion transport and raised sweat chloride 1. The gene is responsible for the production of CFTR protein which functions as a cyclic adenosine monophosphate (cAMP)-dependent chloride channel in epithelial cells, as well as regulating sodium transport in the airways via the epithelial sodium channel (ENaC) 2, 3. Disruption of this protein in CF results in diminished chloride secretion and sodium hyperabsorption, abnormalities which can be assessed by nasal potential difference (PD) measurements 4, 5.
The genetic mutations responsible for CF are classified by their functional capacity with class I to III mutations generally considered as “severe” defects. However, specific genotypes correlate poorly with pulmonary function, and disease heterogeneity exists for individuals with severe mutations 6, 7. Putative mechanisms for this include genetic modifiers and environmental factors 8. Sporadic residual chloride function has also been demonstrated in homozygous ΔF508 (a class II mutation) patients by nasal PD measurement 9–11.
As the pathological manifestations of CF probably result from abnormal epithelial ion transport, it follows that variations in disease expression (and ultimately survival) may be due to variations of CFTR function. We have recently reported 112 CF patients ≥40 yrs of age, of whom 30% were homozygous ΔF508 and many were relatively clinically stable 12, and in this population only limited evidence for environmental influences exist, suggesting that CFTR function variability might be important 13. Some studies have demonstrated that lower baseline nasal PD 4, 14, a decreased response to amiloride 15 and lower sweat chloride concentrations 16 are associated with mutations linked to milder phenotypes (e.g. pancreatic sufficiency) and others have shown that ion transport abnormalities have distinct clinical outcomes 11. No study has yet determined if preserved CFTR function confers a significant survival advantage in patients with “severe” mutations.
In view of the evidence relating CFTR function variability with clinical status and the importance of identifying mechanisms underlying survival advantages, we prospectively evaluated the transepithelial nasal PD and sweat chloride of long-term survivors of CF with severe mutations, hypothesising that their survival advantage was, in part, due to residual CFTR function. Young CF adults with severe and mild lung disease were used as controls and compared with CF adults ≥40 yrs of age; we postulated that the long-term survivors would have CFTR function similar to the young mild group, and both would be significantly better than the young severe group.
METHODS
Subjects
The inclusion criteria for this study were: 1) a definitive diagnosis of CF (characteristic clinical manifestations and confirmatory diagnostic tests) 17; 2) a disease-causing CFTR mutation, class I to III only and on both alleles; 3) aged 18–23 yrs (controls) or ≥40 yrs (long-term survivors). Lung function (forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC)) was collected retrospectively for all patients so that the younger group could be subdivided into terciles by FEV1. It was taken from their most recent annual review assessment (i.e. within 12 months). This had been performed during clinical stability, using a standard spirometer (Jaeger, Würzburg, Germany) and expressed as % predicted for age, sex and height using published reference values 18. Of the young patient group, only those in the lower and upper FEV1 terciles were recruited. There were no lung function restriction criteria for the older group. Patients were excluded from PD measurements if they had nasal polyposis (n = 1) or recent nasal surgery (n = 1). The measurement was deferred if they had an acute upper respiratory tract infection/rhinitis (by 1 month after full symptom resolution). Informed, written consent was obtained from all participants. The study was approved by the Royal Brompton Hospital Research Ethics Committee (London, UK).
Nasal PD and sweat chloride
Nasal PD measurement was performed by a single operator using the method described by Middleton et al. 19. The integrity of the silver/silver chloride electrodes was verified by measuring finger PD. PD measurements were performed with perfusion of solutions at room temperature in the following sequence: 1) maximal (most negative) stable baseline PD in the presence of a buffer solution (HEPES); 2) perfusion with amiloride (change in PD in the presence of amiloride (ΔAmil)); 3) perfusion with a low chloride solution (change in PD in the presence of a low chloride solution (Δlow Cl-)); and 4) perfusion with isoprenaline (Iso) in a low chloride solution. These stages represent sodium channel-mediated sodium hyperabsorption (1 and 2), hyperpolarisation via chloride secretion occurring down an electrochemical gradient (3) and activation of cAMP-dependent chloride (CFTR) channels (4). Steps 3 and 4 together measure the change in PD in the presence of low chloride solution followed by low chloride/Iso solution (ΔlowCl- + Iso). To take into account both the sodium and chloride elements of the nasal PD measurements, the Wilschanski index was calculated (index = eresponse to low chloride solution and isoprenaline/response amiloride) 20; a cut-off >0.70 predicts CF. The nostril with the highest (most negative) baseline was studied. For internal consistency, PD measurement was repeated in the same nostril at the point of highest baseline and at least 6 h apart (duration chosen to allow the dissipation of residual amiloride and Iso based on prior experiments (unpublished data)). Two sweat tests were performed using the Macroduct system 21 and analysed using a titrimetric assay with silver nitrate reagent. They were both performed on the same day (which was the same day as the first nasal PD measurement) under identical conditions.
Clinical data
Body mass index (BMI) was taken from the patients' most recent annual review record. BMI and spirometry were also taken from the first available records of the old group (i.e. when they would have been a similar age to the young groups). The remaining clinical information was taken from the CF database of the Royal Brompton Hospital (London, UK): pancreatic insufficiency (low faecal elastase; <200 μg·g−1), CF-related diabetes (CFRD) (based on oral glucose tolerance test and serial glucose monitoring); and sputum microbiology (chronic infection, 75% of sputum samples positive for the organism over the previous 12 months based on more than four samples).
Statistical analysis
A sample size of 34 patients in each group provides 80% power testing at the 5% significance level using one-way ANOVA to compare the baseline nasal PD between the three groups (based on expected baseline±sd values of -35±9 mV (young/severe) and -29±9 mV (young/mild and old)). Patient permitting, nasal PD and sweat chloride measurements were repeated to reduce intra-subject variability. If repeat measurements were performed, the arithmetic mean for each patient was calculated. Differences in nasal PD and sweat test measurements were tested by Kruskal–Wallis (for non-parametric data) and then if significant, by Dunn's multiple comparison. Fisher's exact test was used to compare categorical variables. Linear regression models were used to assess the relationship between continuous variables. Multivariate analyses were performed with FEV1, BMI, Pseudomonas aeruginosa status and age as independent variables. A paired t-test was used to assess the change in BMI and spirometry in the old group from the first to most recent assessment. A p-value of <0.05 was considered to be statistically significant.
RESULTS
Clinical characteristics
Nasal PD measurements and sweat chloride concentrations were prospectively measured for 94 patients with CF. The clinical characteristics of each group are presented in table 1. Older patient data are presented as the most recent and the first recorded value (at mean±sd age 22.8±8.1 yrs, i.e. similar to the young groups, mean±sd age 21.1±1.8 yrs). 76 (80.9%) patients were homozygous ΔF508 and the remainder were ΔF508 compound heterozygotes (with genotype G551D (n = 5), G542X (n = 3), N1303K (n = 3), 1717-1G→A (n = 2), 621-1G→T (n = 1), R1162X (n = 1), 2789+3delG (n = 1), 3659delC (n = 1) and D1507 (n = 1)); no significant difference between the groups for any genotype was present.
BMI was lowest in the young/severe group (table 1). In the older group, there was a significant (p<0.001) increase in BMI and decline (p<0.001) in FEV1 over the period from the first recorded to the most recent value (mean±sd) 23.0±7.9 yrs (table 1). First recorded FEV1 was significantly (p<0.001) greater than the young/severe group but lower (p<0.05) than young/mild group. First recorded BMI was similar to the young/severe group and significantly (p<0.01) lower than the young/mild group.
Neither sex ratio (65% male) nor pancreatic status was different across the groups. Significant differences were seen with respect to frequency of CFRD (more common in the old versus young/mild group, p = 0.005) and chronic infection with P. aeruginosa (more common in the old and young/severe versus young/mild group; p<0.05 and p<0.005, respectively).
Nasal PD measurements
A total of 153 nasal PD measurements were performed (93+60 repeat measurements (n = 23, old; n = 19, young severe; and n = 18, young/mild)). Ion transport measurements for each group are shown in figure 1. Baseline PD was not significantly different across the three groups. ΔAmil was significantly different across the three groups (p = 0.01, Kruskal–Wallis); the older group had values which were not significantly different to either young group but the young/severe group had higher values than those in the young/mild group (p<0.01). The responses to ΔlowCl- + Iso were minimal; hyperpolarisation (i.e. towards normal (more negative)) did not exceed a mean of 1.2 mV in any group (with no significant difference between the groups). ΔAmil values remained significantly different (p<0.05) between the young/mild and young/severe group, and the ΔlowCl- + Iso response was unchanged when analysed separately for both sexes (data not shown).
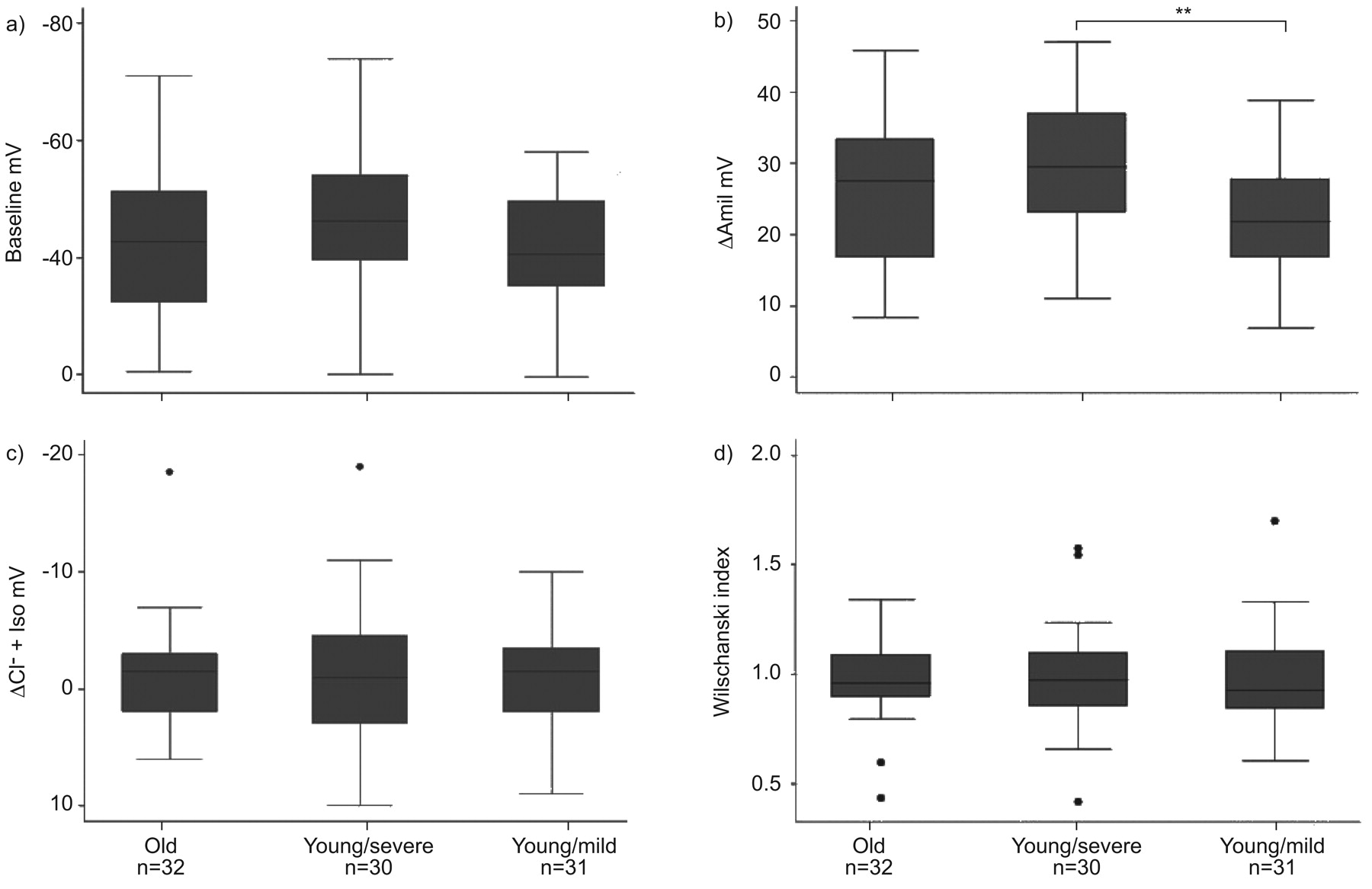
Box plots demonstrating the range and variability of nasal potential difference (PD) measurements. a) Baseline; b) change in PD in the presence of amiloride (ΔAmil); c) change in PD in the presence of low chloride solution followed by low chloride/isoprenaline solution (ΔlowCl- + Iso); and d) Wilschanski index (eresponse to low chloride solution and isoprenaline/response amiloride) for each group. The values were significantly different across the three groups (p = 0.01, Kruskal–Wallis) for ΔAmil only; the older group had values which were not different to either young group but the young/severe group had higher values than those in the young/mild group. Boxes show the median and interquartile range (IQR). Whiskers show the highest and lowest data points within 1.5 IQR of the upper and lower quartile. •: outliers outside of these limits. **: p<0.01.
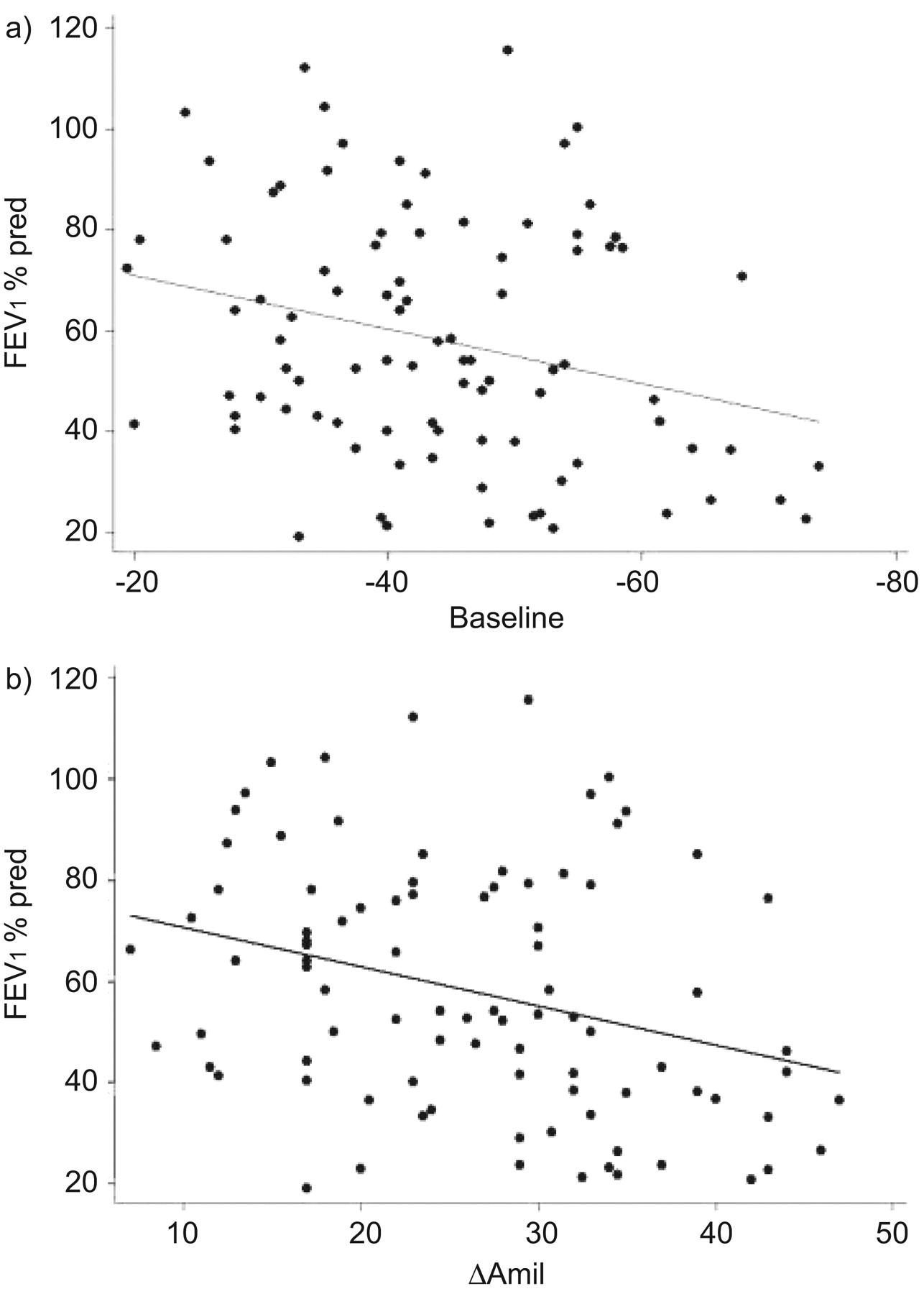
On univariate analysis, baseline PD and ΔAmil (of all three groups) were both significantly associated with FEV1 (fig. 2), with coefficients (95% CI) -0.13 (-0.23– -0.03); p = 0.009 and -0.12 (-0.20– -0.04); p = 0.003, respectively. ΔlowCl- + Iso was not associated with lung function and no PD measurement was associated with age or BMI on univariate analysis. When multivariate analysis was performed, FEV1, but not age, BMI or P. aeruginosa status were related to ion transport measurements (table 2).
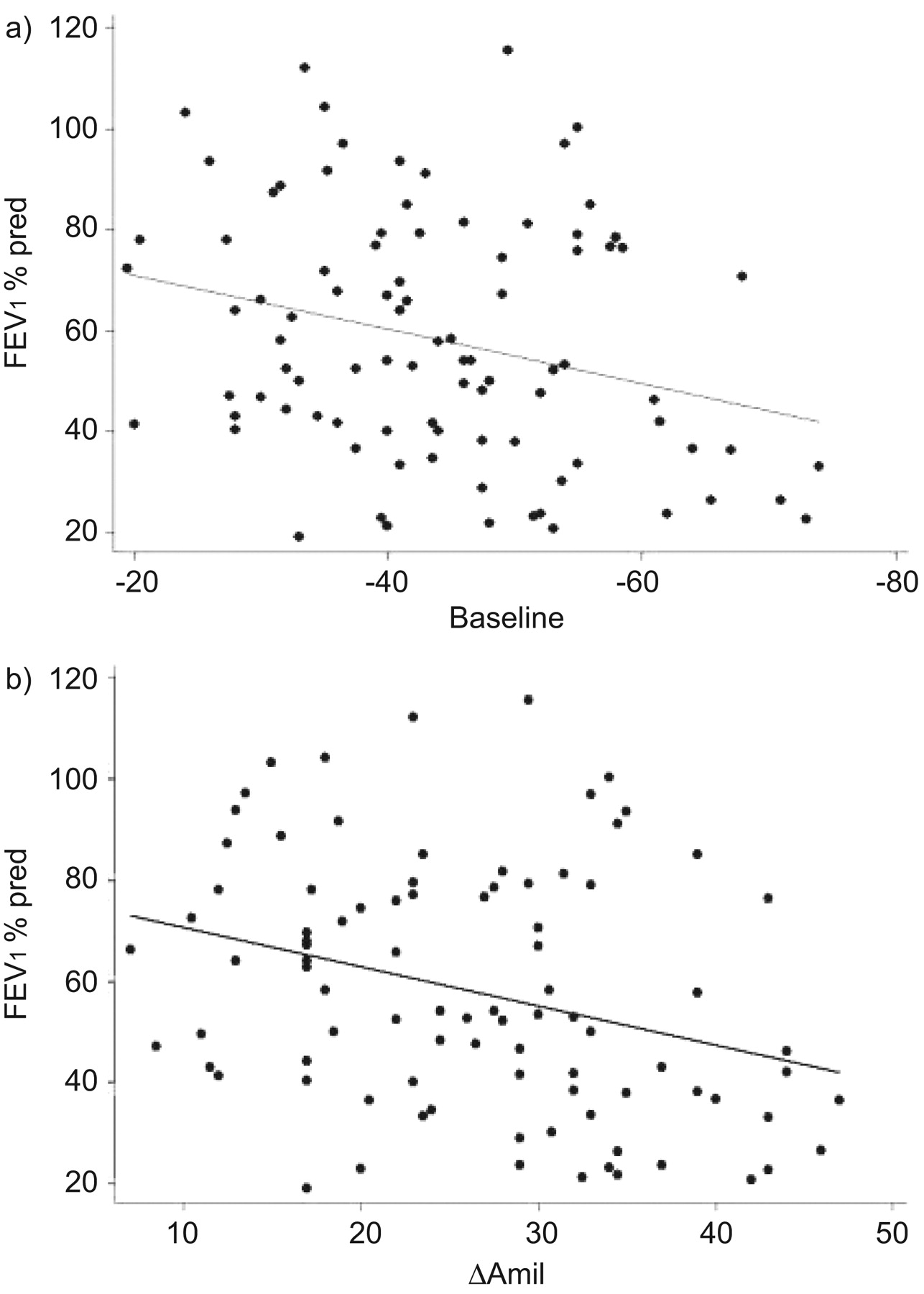
Association of a) baseline potential difference (PD) and b) change in PD in the presence of amiloride (ΔAmil) with forced expiratory volume in 1 s (FEV1) on univariate analysis with coefficients (95% CI) -0.13 (-0.23– -0.03); p = 0.009 and -0.12 (-0.20– -0.04); p = 0.003, respectively. % pred: % predicted.
Patients with significant chloride secretion
Seven patients demonstrated hyperpolarisation of at least 5 mV (ΔlowCl- + Iso) and, of those, three were over 10 mV, indicating chloride secretion well into the recognised “normal” range 22. One of the three had a repeat measurement and ΔlowCl- + Iso remained significantly high (-18 and -19 mV). The characteristics of the three patients are summarised in table 3.
Sweat tests
Sweat chloride concentrations for each group are shown in figure 3. A total of 177 sweat tests were performed (91+86 repeat measurements). Sweat chloride concentrations were significantly different across the three groups (p<0.05, Kruskal–Wallis); the young/mild group had values which were significantly higher (p<0.05) than the young/severe group. On univariate analysis, sweat chloride concentration (of all three groups) was associated with FEV1 (coefficient (95% CI) 0.74 (0.20–1.29); p = 0.008), FVC (0.62 (0.15–1.10); p = 0.011) and BMI (0.16 (0.08–0.24); p<0.001), but not with age or nasal PD. On multivariate analysis, only BMI was associated with sweat chloride. The intra-subject variability with 95% limits of agreement for sweat chloride and nasal PD measurements is shown in table 4.

{kind=link}
{kind=link}
{kind=link}
Box plot demonstrating the range and variability of sweat chloride concentrations for the three groups (p<0.05; Kruskal–Wallis); the young/mild group had values which were significantly higher (*: p<0.05) than the young/severe group. Boxes show the median and interquartile range (IQR). Whiskers show the highest and lowest data points within 1.5 IQR of the upper and lower quartile. •: outliers outside of these limits.
DISCUSSION
This prospective study of in vivo CFTR function in long-term survivors of CF with severe mutations demonstrates that neither nasal ion transport nor sweat chloride were associated with increased survival. However, there was an association between nasal PD and pulmonary disease severity, although this related only to sodium and not to chloride transport.
The explanations for these findings are likely to fall into two main categories. First, the study hypothesis relies on the fact that disease heterogeneity in patients with similar genotypes results primarily from factors influencing CFTR function. While it is well recognised that disease severity can vary greatly for identical mutations, it is also recognised that concordance is greater in monozygotic twins than dizygotic twins 23. This indicates that “environmental” factors (e.g. time of diagnosis and adherence to treatment) cannot be exclusively responsible for this variability and other genetic influences are likely. Since over 200 polymorphisms have been identified within CFTR itself 24, it is likely that some will interfere with its function, evidence for which is accumulating 25. If factors such as these influence disease outcome then they were either under-represented or not influential enough in the older patient group, although they may provide some explanation for the patients who had evidence of preserved chloride secretion.
The other plausible explanation for the results from the present study relates to the characteristics of the groups studied. To investigate the relative differences in transepithelial ion transport a comparison was made with a significantly younger group with extremes of lung function (i.e. a surrogate marker of severity itself). Ion transport abnormalities are probably responsible for the abnormal airway environment which triggers the cycle of infection and inflammation, but whether or not it continues to drive this response is less clear. CFTR function was measured in the old group at an age that may have been many years after the initiation of this cycle and therefore may be less relevant to their survival. We also have made the assumption that the young patients with better lung function will themselves be long-term survivors, which of course can only be proven in 20 yrs time. Our study showed no correlation between age and measurements of ion transport but others have suggested that baseline PD decreases and sweat electrolytes increase as a function of age in CF 4, 11; further longitudinal studies are therefore required to evaluate this relationship.
The study was designed to assess whether patients with severe mutations have a survival advantage due to residual CFTR function and, therefore, by inclusion criteria, only patients with class I to III CFTR mutations were included. Thus it may be argued that, by definition, a significant chloride secretory response was not going to be demonstrated. However, the rationale for restricting the study to this genotype was three-fold: 1) evidence of sporadic function exists in the literature for patients with such genotypes 9–11, and our results also confirmed this (table 3); 2) studies have shown that homozygous ΔF508 genotype can be associated with long-term survival and this may be due to variation in CFTR function, not environmental influences 12, 13; and 3) increasingly the importance of ENaC and sodium transport on CF-like lung disease is being recognised 26. This may also be directly relevant to CF, as differences in the level of interaction between ENaC and CFTR may explain differences in the expression of the disease and variability of survival. The study was powered to detect differences in baseline PD and therefore by restricting genotype we hoped to find evidence of these differences in CF.
So what do these findings add to what is already known? First, they demonstrate that patients surviving for more than 40 yrs with CF do not have preserved CFTR function at that time-point compared with young patients. An association of lung function with ΔAmil was confirmed 11, but not with baseline PD, which has been demonstrated in previous studies 4, 14, although not consistently 27. The chloride secretory response did not correlate with FEV1 or FVC, which is in contrast to findings from a study of ΔF508 homozygous sibling pairs 28 and a study showing residual function in males 10. A recent study has demonstrated that the phenotype of airway transepithelial ion transport is a continuum and strongly associated with CFTR genotype 29. Our study is consistent with this as we did not detect significant variations in CFTR function, presumably due to lack of genotype heterogeneity, but in line with their findings, sodium transport appears to be an important predictor of clinical phenotype, lending support to the ENaC hypothesis 26. Our study also lends support to the presence of other important survival factors, independent of the initiating insult and ion channel abnormalities. One such factor is BMI; a striking finding was that BMI increased significantly in the old group between the ages of 20 and 40 yrs in spite of a significant decline in lung function, more P. aeruginosa and more CFRD. Interestingly, BMI of the long-term survivors at 20 yrs of age was similar to the young severe group, despite lung function that was intermediate (i.e. between the young severe and mild groups) at that time. This suggests that survival for the mild group may exceed the older group which is in keeping with the steady increase in survival for each cohort of patients over the past few decades 30. This is encouraging, but also serves to highlight the need for effective healthcare planning for the future as adult CF clinics continue to expand.
The sweat chloride results from the present study were unexpected, revealing a lower chloride concentration in the young/severe patients compared with the young/mild and older patients. Previous attempts to correlate sweat electrolytes with lung disease severity have been unsuccessful, citing random variation or environmental factors as possible explanations 16, which may also have been important in our study. As the nasal PD values did not correlate with sweat chloride values in our study, it suggests that an undetermined mechanism may have interacted with the sweat physiology or, perhaps more probable in our opinion, that the sweat result was spurious and a result of a type I statistical error. Further limitations of our study might include the unequal sex distribution, as there is some evidence to suggest that nasal PD varies with menstruation 31. In addition, the prevalence of P. aeruginosa infection was highest in the young severe group, the multivariate analysis from our study showed this variable was not associated with measures of ion transport, although others have demonstrated that this association may exist 15. The intra-subject variability of nasal PD and sweat chloride measurements warrants acknowledgement. The mean difference and limits of agreement (table 4) show variability was present, particularly for measures of chloride secretion, and although this would have resulted in some loss of power, the variability was similar to other published studies 32.
This is the largest study of nasal PD measurements in “old” CF patients to date. By using an age criteria of ≥40 yrs and specific genotypes, we identified a unique subset of CF patients who had lived beyond the current median life expectancy of approximately 38 yrs, which is not explained by “mild” mutations. Our findings indicate that long-term survival cannot be explained by residual CFTR function when measurements (nasal PD and sweat chloride) are taken in later life. This has important implications for other factors, such as BMI, which we postulate was one of the most significant influences of survival in this group 13. Without onerous longitudinal studies to determine if patients with residual CFTR function and better lung function exceed life expectancy, we suggest that predictions of survival based on nasal PD and sweat test measurements should not be made.
Footnotes
Statement of Interest
None declared.
- Received May 20, 2010.
- Accepted August 18, 2010.
- ©2011 ERS
REFERENCES










