





Abstract
The typical radiographical findings of cytomegalovirus pneumonitis are bilateral interstitial infiltrates.
In this study, the current authors describe two patients on corticosteroid treatment for systemic lupus erythematosus, complicated by histologically confirmed cytomegalovirus pneumonitis, presenting as cavitary masses.
This rare presentation of cytomegalovirus pneumonitis broadens the differential diagnosis of cavitary lesions to include cytomegalovirus infection in immunocompromised individuals.
Cytomegalovirus (CMV) is a well-recognised cause of morbidity and mortality in patients with impaired cellular immunity. Radiographical manifestations of CMV infection are variable, and include interstitial infiltrates, focal or diffuse pulmonary opacification and nodules 1. In this study, the authors report two cases of histologically proven episodes of CMV infection presenting as cavitary masses.
Case 1
A 34‐yr‐old female presented with renal failure requiring haemodialysis. A renal biopsy was consistent with lupus nephritis World Health Organization (WHO) class IV. Systemic lupus erythematosus (SLE) was diagnosed and the patient received 1 g of methylprednisolone for 3 days, followed by oral prednisone.
A week later, she developed fever and chest radiography revealed new bilateral infiltrates. Computerised tomography (CT) of the chest revealed bilateral peripheral parenchymal infiltrates and a cavitating mass measuring 5×3 cm in the right lower lobe. Multiple blood, urine and sputum cultures were negative, and fibreoptic bronchoscopy was nondiagnostic. The patient continued to be febrile, despite initiation of broad-spectrum antibiotics. Transoesophageal echocardiogram did not reveal vegetations and CT‐guided transthoracic lung biopsy of a cavitary lung mass was unrevealing. The patient remained febrile and a repeated CT of the chest demonstrated progressive cavitation with thinning of the cavity walls (fig. 1⇓). She underwent thoracoscopic lung biopsy with wedge resections of both right upper and lower lobes, which revealed a florid CMV infection. Histological findings included numerous intranuclear and intracytoplasmic inclusions, associated with interstitial fibrosis and intra-alveolar haemorrhage (fig. 2⇓). No bacterial, mycobacterial or fungal organisms were identified and cultures of the pulmonary tissue only grew CMV. A CMV antigenaemia assay was positive and CMV isolation in blood was confirmed by immunofluorescence assay. A diagnosis of CMV infection was made and i.v. ganciclovir and i.v. immunoglobulin (Ig)G were initiated, followed by clinical improvement. After 5 weeks, a follow-up chest CT scan revealed a smaller right lower lobe cavity with resolution of the surrounding infiltrates (fig. 3⇓).
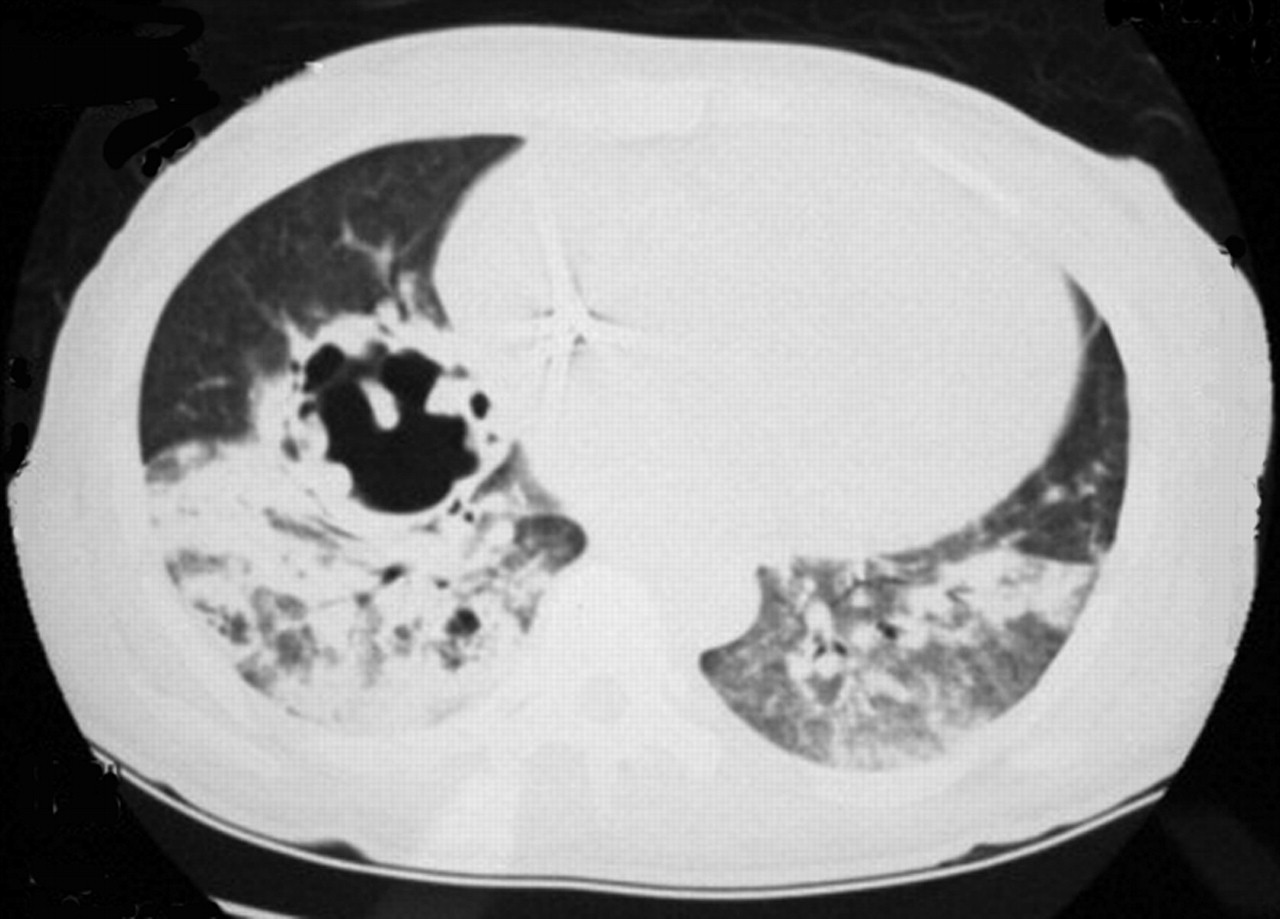
Helical computerised tomography scan of chest, using 5‐mm collimation of the lung, showing bilateral lower lobe consolidation with cavitation in right lower lobe.
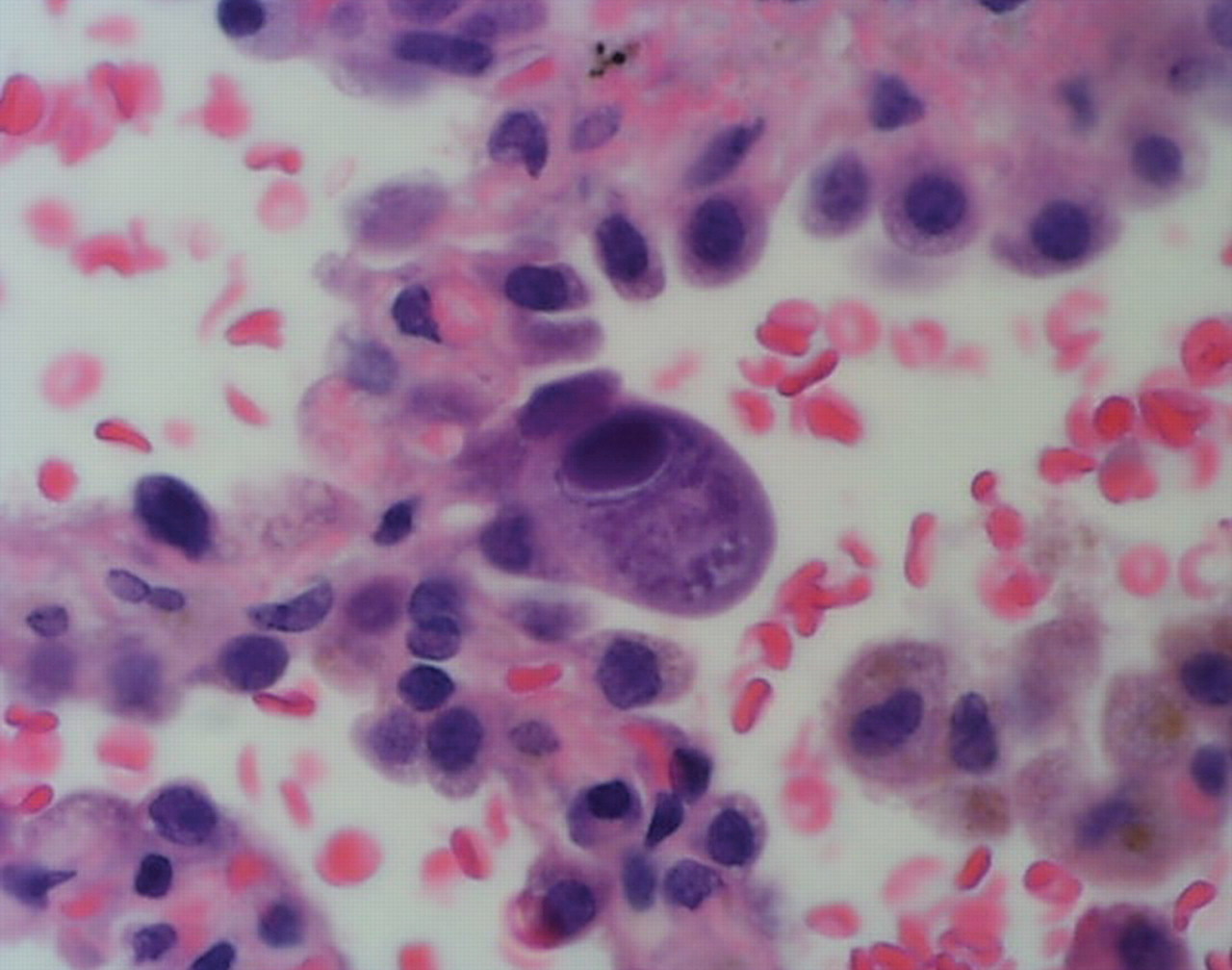
High-power photomicrograph (haematoxylin-eosin stain) ofsurgical lung biopsy specimen shows numerous cytoplasmic andintranuclear cytomegalovirus inclusion bodies in alveolar pneumocytes.
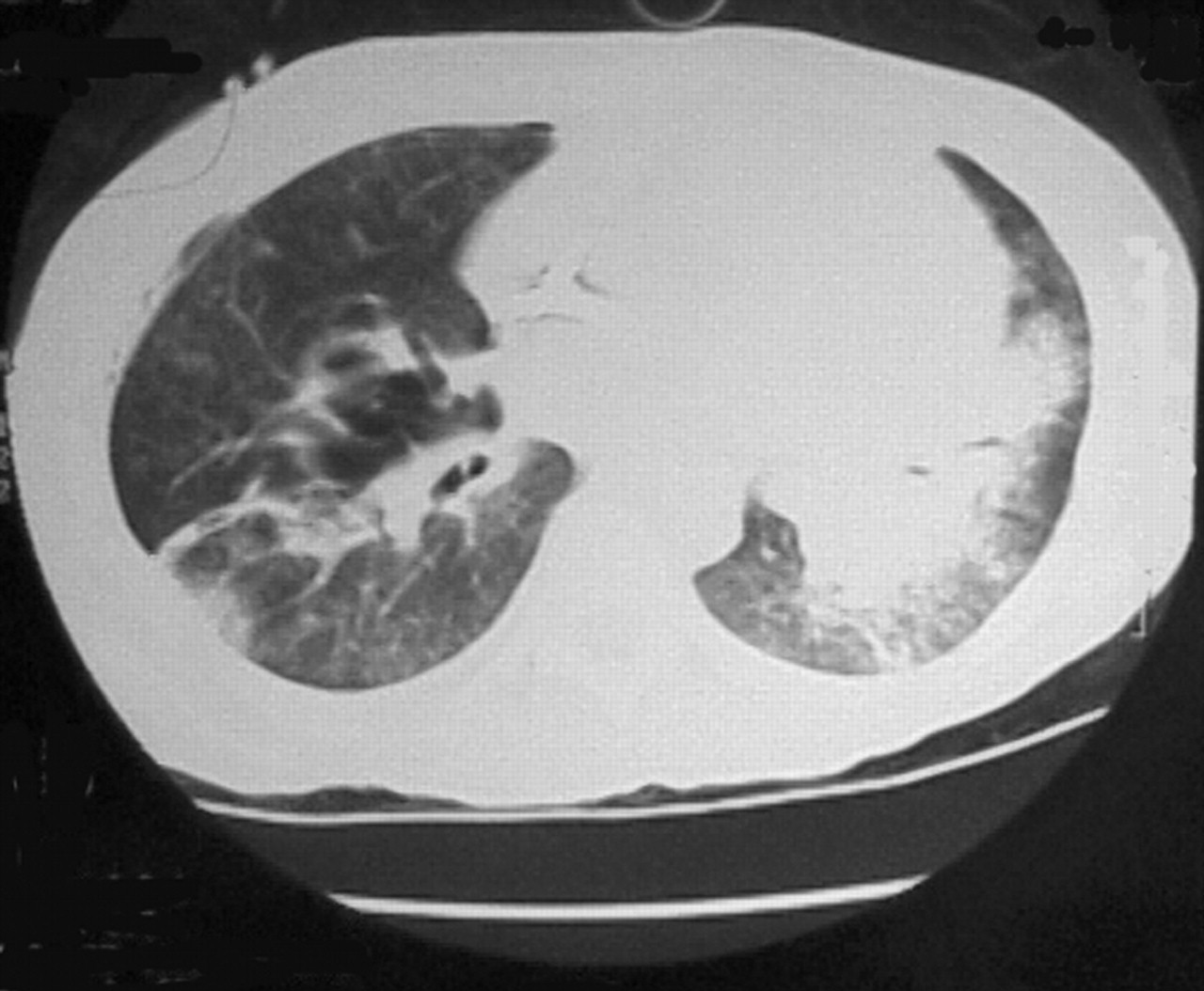
Helical computerised tomography scan of chest using 5‐mm collimation of the lung showing smaller right lower lobe cavity with resolution of surrounding infiltrates.
Case 2
A 33‐yr‐old male with SLE, complicated by WHO class‐IV lupus nephritis, was hospitalised with fever, dyspnoea and worsening renal function. He had been treated with chronic steroid therapy, azathioprine and multiple cycles of cyclophosphamide. Positive blood cultures for Streptococcus pneumoniae prompted treatment with ceftriaxone. He also received 3 days of q.d. 1 g methylprednisolone, followed by oral prednisone. He developed a fever 6 weeks later and CT of the chest revealed a right upper lobe thick-walled cavitary lesion (fig. 4⇓). As bronchoscopy was unrevealing, the patient underwent surgical wedge resection of the right upper lobe cavitary lesion. On pathology, there was evidence of focal interstitial fibrosis, accumulation of intra-alveolar macrophages, and CMV with intracytoplasmic and nuclear inclusions in the lining alveolar cells. No bacterial, mycobacterial or fungal organisms were seen or cultured. Serology revealed CMV IgM >1.20 (<0.70) and CMV IgG >400 (<4). A diagnosis of CMV pneumonitis was made and ganciclovir treatment was initiated with clinical improvement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Helical computerised tomography scan of chest using 5‐mm collimation of the lung showing a thick wall cavitary lesion in the right apex measuring 3.8×3.6×3.5 cm contiguous with the pleura.
Discussion
Here, the current authors report two histologically proven cases of cavitary lung lesions, solely attributed to CMV infection. This is a unique description of CMV cavitary disease in patients on high-dose corticosteroid therapy for SLE. In these cases, there was no evidence of active vasculitis, neoplasm, or bacterial, mycobacterial and fungal infection. Only CMV, with its pathognomonic intranuclear and intracytoplasmic inclusions, was identified.
The usual extensive differential diagnosis of cavitary masses in immunocompromised hosts includes bacterial, tuberculous, fungal and Pneumocystis carinii infections, septic emboli, and malignancy. These cases demonstrate that it must now encompass CMV infection.
CMV pneumonitis is usually suggested by the presence of fever, hypoxaemia and nonproductive cough in an immunocompromised host. The radiographical appearance is variable and includes interstitial infiltrates, ground glass attenuation, consolidation and pulmonary nodules 1–3. Cavitary lesions associated with CMV infection are extremely rare and were previously attributed to polymicrobial infection. Furthermore, in previous studies, CMV was detected by bronchial wash only, which does not confirm active infection 4. Aviram et al. 4 reported 20 cases of AIDS with cavitary lung disease and identified CMV as the sole pathogen in only one patient, however, without elucidating the basis for this conclusion. In another study of 21 patients with AIDS with CMV infection, only one had a thick-walled cavitary lesion on CT of the chest, which was attributed to Pneumocystis carinii infection 5. In 21 episodes of CMV pneumonia occurring after bone marrow transplantation, the most common radiographical findings were pulmonary opacification and nodules, but there were no reports of cavitary lesions 1. The radiographical manifestations of 15 episodes of symptomatic CMV pneumonitis following lung transplantation included diffuse (60%) and focal (33%) parenchymal haziness and focal consolidation (7%) 6. The only case of histologically proven (open lung biopsy) CMV pneumonia, presenting as a cavitary mass, occurred in an immunocompetent patient 7.
In conclusion, the differential diagnosis of cavitary lesions in immunocompromised patients should include cytomegalovirus pneumonitis, especially as effective antiviral treatment is available.
- Received October 8, 2003.
- Accepted February 2, 2004.
- © ERS Journals Ltd









