





Abstract
The aim of the current study was to assess the safety of bronchoscopy-guided radiofrequency ablation (RFA) and compare the effectiveness between new internal cooled-RFA and standard noncooled-RFA.
Normal lungs from sheep were used (n = 6). Internal cooled-RFA and standard noncooled-RFA were set to assess the most suitable RFA conditions, such as power output, flow rate and ablation time. Internal cooled-RFA was then applied under the most optimal conditions of power output and flow rate for 15, 30, 60 and 120 s, and two water temperatures either room temperature (RT) water or cold water. Criteria for the most appropriate conditions were set over 15 s of ablation time and 50°C of the tip's temperature.
Internal cooled-RFA had no complications. Standard noncooled-RFA was complicated with bronchial bleeding after RFA. On the basis of the histological findings, average temperature and average output, the most appropriate conditions of the cooled-RFA were a power output of 30 W and flow rate of 30 or 40 mL·min−1. The cooled-RFA using cold water caused a smaller, more discrete, lesion compared with that using RT water.
Bronchoscopy-guided internal cooled-radiofrequency ablation was an effective, safe and feasible procedure that could become a potential therapeutic tool in managing lung pathology.
- Fibreoptic bronchoscopy
- internal cooled-radiofrequency ablation
- radiofrequency ablation
- standard noncooled-radiofrequency ablation
Radiofrequency ablation (RFA) uses an electromagnetic wave with a frequency band the same as an electric scalpel used in surgery and a radiofrequency interchange electric current. RFA is a new treatment offered as a minimally invasive treatment and is most commonly used to treat patients with liver tumours 1, kidney cancer 2, breast cancer 3 or lung cancer 4. Tumour cells are generally more susceptible to heat than normal cells. This procedure is safe, technically feasible and suitable for use with imaging guidance technologies, such as ultrasonography, radiograph and computed tomography (CT).
Mortality from lung cancer remains high and establishment of new therapeutic modalities are needed. RFA has been described as a new technique for the treatment of lung cancer, and Miao et al. 5 suggested that cooled-RFA is an effective alternative to lobectomy, in certain patients, for the minimally invasive treatment of lung cancer. In the USA, standard RFA has been more widely used than percutaneous imaging-guided therapy 6. Complications from this method include pain, pneumothorax, haemothorax and pleural effusion 7. Tsushima et al. 8 reported fibreoptic bronchoscopy-guidance under real-time CT fluoroscopy for the diagnosis of peripheral lung lesions. A critical aspect is that this procedure may reduce the above complications if RFA can be applied using real-time chest CT images under fibreoptic bronchoscopy.
The current authors developed a new internally cooled electrode (Japan Application No. 2006-88228) suitable for forceps channel bronchoscopy. The initial aim of the present study was to compare the effective differences between the new internal-cooled electrode and the standard noncooled electrode and to assess the feasibility and safety of bronchoscopy-guided RFA using normal sheep lungs.
METHODS
Ethical considerations
The study protocol was approved by the Institutional Review Board for the care of animals at Shinshu University (Asahi, Matsumoto, Japan). The care and handling of animals was in accordance with the guidelines of the National Institute of Health. The animals had free access to commercial food and drinking water.
Preparation
Ex vivo RFA was performed on six male sheep (weight 35–50 kg) in the Shinshu University animal care facility. They were fasted for 8 h before fibreoptic bronchoscopy to prevent aspiration pneumonia. The sheep were anaesthetised using intravenous probocol (10 mL bolus) and an 8.0-mm tracheal tube was inserted after cutting part of the anterior trachea. Their limbs were fixed to the table in the supine position and spontaneous breathing was maintained under anaesthesia with probocol (0.5 mL·min−1). RFA was performed in the animal operation room under radiograph fluoroscopy (BV-25 Gold; Philips, Linton, UT, USA).
Fibreoptic bronchoscopy
After airway anaesthesia with 2% lidocaine hydrochloride, the sheep underwent fibreoptic bronchoscopy. Supplemental oxygen during the procedure was not needed. A flexible fibreoptic bronchoscope (Olympus; Tokyo, Japan), BF 1T20 (outer diameter; 5.0 mm, forceps channel; 2.2 mm) was inserted via the tracheal cannula route under local anaesthesia.
RFA preparation
Two kinds of electrode were prepared for RFA: an internal cooled-electrode with a 4-mm active tip (fig. 1a⇓; ablation tip: 4 mm, diameter: 1.67 mm; Shinshu University) and a standard noncooled-electrode with a 4-mm active tip (fig. 1b⇓; ablation tip: 4 mm, diameter: 1.67 mm; Shinshu University). These electrodes were attached to a monopolar radiofrequency generator (Shinshu University) able to produce 50 W as the maximum output. Tissue impedance was monitored continuously by a generator and an impedance-controlled radiofrequency algorithm was used. During the RFA procedure, a thermometer embedded within the electrode tip continuously measured the temperature and its upper limit was set at 70°C. Grounding was achieved by attaching one or two standard steel mesh dispersive electrodes to the sheep's abdomen. A peristaltic pump (Shinshu University) was used to infuse water into the internal lumen of the catheter electrode at several rates (20–50 mL·min−1). When the desired power output could not be applied as a result of the elevation of impedance due to tissue boiling, the generator automatically switched off the electrode. Current pulsing was also performed manually to avoid charring of local tissue caused by the rapid increase of impedance, which limited further heat diffusion.

a) An internal cooled radiofrequency ablation electrode. b) Tip of the electrode. Only a 4 mm-tipped electrode produced power output, the tip temperature and impedance were measured.
RFA procedure
Various conditions were set to assess the most suitable RFA condition according to the methods of cardiac conduction abnormality for procedure 1 9–11. An X-ray fluoroscopic image was obtained to correlate the location of the electrode tip in peripheral lung lesions with ∼1-cm margin from pleura to prevent pneumothorax complications. Once the appropriate peripheral location of the electrode tip was confirmed and impedance was <300 Ω, RFA was used. The settings regarding the areas which were ablated were as follows.
Procedure 1: To compare between standard noncooled-RFA and internal cooled-RFA, standard noncooled-RFA (power output; 30 W) ablated each right lobe only once and internal cooled-RFA (power output; 30W, flow rate 30mL·min−1) ablated each left lobe only once. RFA was initially applied for 120 s under several conditions of power output and flow rate (table 1⇓). Lungs from one sheep were harvested to assess ablated areas macroscopically and histologically immediately after ablation.
Procedures of radiofrequency ablation(RFA)
Procedure 2–1: To obtain an optimal output of 30 W, several sets of flow rates were performed. Internal cooled-RFA with flow rates of 20, 30 and 40 mL·min−1 were ablated once in the upper, middle and lower lobes, respectively. One sheep was harvested immediately and another harvested 7 days after ablation.
Procedure 2–2: Different output (20 W and 40 W) and flow rate (20, 40 and 50 mL·min−1) parameters were used to compare the data at 30 W. Internal cooled-RFA was ablated once in each right lobe and left lobe using a power output of 20 and 40 W, respectively. Lungs obtained from one sheep were harvested at 7 days after ablation.
Procedure 3: Internal cooled-RFA was applied under the most optimal conditions of power output and flow rate for 15, 30 and 60 s, using two different temperatures of flow water (room temperature water or cold (4°C) water). Internal cooled-RFA was used once for 15, 30 and 60 s in the upper, middle and lower lobes, respectively. Two sheep were harvested 7 days after ablation. Internal cooled-RFA was performed on the bronchial mucosa using the same methods as described previously.
Histopathological analysis
Two sheep were sacrificed immediately and four 7 days (n = 4) after the RFA procedure using an overdose of ketamine. Their lungs were then harvested. Gross examination for bronchial haemorrhage, atelectasis and perforation was performed on all sheep. For microscopic examination, two observers measured the central discoloured region of coagulation necrosis in each pathological specimen and the average was calculated. Tissues were fixed in 10% formalin for routine histological processing with paraffin sectioning and haematoxylin-eosin staining for light microscopic examination.
Data analysis
Technical assessment, therapeutic efficacy and RFA complications were analysed. Changes in the morphology and attenuation of the lesion after RFA were recorded. Optimal conditions were based on complications, local tissue temperature, histology and procedure time in conjunction with power output, flow rate and impedance data. The above criteria were assessed with >15 s of ablation time and the temperature of the electrode at 50°C as a prolonged ablation exposure could have denatured lung tissue due to generation of high temperatures.
RESULTS
As shown in figure 2⇓, a standard noncooled-RFA was continued for up to 120 s. It was complicated with bronchial bleeding immediately after RFA. Impedance increased from 770 to 999 Ω. Macroscopic findings showed bronchial haemorrhage and necrosis of 25×15 mm. Standard noncooled-RFA showed diffuse bronchial bleeding from all ablated lobes. All histological findings showed diffuse alveolar haemorrhage, lung oedema and destruction of the alveolar space. It was concluded that, despite achieving a sufficient area of coagulation necrosis, this electrode was not suitable for lung ablation because of the increase of impedance and bronchial haemorrhage.

Radiofrequency ablation for 120 s using a standard noncooled electrode with a power output of 30 W. a) Low power output (mean 1 W and maximum 3 W), b) temperature (mean 68°C and maximum 76°C) and c) impedance (increased from 770 to 999 Ω). d) Macroscopic findings showed large coagulation necrosis. e) Microscopic findings showed diffuse alveolar haemorrhage, destruction of alveolar space (haematoxylin-eosin stain; scale bar = 0.5 mm).
Internal cooled-RFA had no immediate complications. As shown in figure 3⇓, the average temperature of 20 W power output decreased slightly according to the flow rate. With a power output setting of 20 W and a flow rate of 20 mL·min−1, impedance increased from 300 to 999 Ω. Histological findings showed diffuse alveolar haemorrhage and preserved structure of the alveolar space. With a flow rate of 40 mL·min−1, histological findings did not differ from those with a flow rate of 20 mL·min−1 (table 2⇓).

Radiofrequency ablation for 120 s using an internal cooled electrode with a power output of 20 W and flow rate of 20 mL·min−1. a) Power output (mean 16 W and maximum 18 W), b) temperature (mean 43°C and maximum 56°C) and c) impedance (increased from 300 to 999 Ω). Wide wave range meant changes accompanied deep breathing. d) Macroscopic findings showed a ring burn and normal central area. e) Microscopic findings showed some haemorrhage and maintenance of the alveolar space (haematoxylin-eosin stain; scale bar = 0.5 mm).
Radiofrequency ablation parameters
As shown in figure 4⇓, with a power output setting of 30 W and a flow rate of 40 mL·min−1, impedance decreased from 174 to 97 Ω. Macroscopic findings showed necrosis of 15×15 mm, and no bronchial bleeding. Histological findings showed diffuse alveolar haemorrhage and necrosis. With 30 W power output and a flow rate of 20 mL·min−1, sufficient power output could not be achieved because of the rapid increase in the tip's temperature; however, histopathological findings showed the same lesion and size as with a flow rate of 40 mL·min−1. The findings between a flow rate of 30 and 40 mL·min−1 were almost identical (table 2⇑). Although not illustrated by the data, when using a 40 W power output, the temperature of the electrode tip reached 60°C; therefore, the flow rate remained high because the tip temperature rapidly increased with a low flow rate. Impedance decreased from 245 to 189 Ω. Histological findings showed diffuse alveolar haemorrhage, lung oedema and destruction of the alveolar space. A power output of 40 W achieved almost the same size of coagulation necrosis as 30 W, for clinical safety; therefore, a 40 W power output is suggested to be unnecessary for ablation of the lung tissue. On the basis of these histological findings and the average temperature and output, the most appropriate conditions for the cooled electrode were a 30 W power output and a flow rate of 30 or 40 mL·min−1. In addition, the temperature of the electrode tip needed to ablate the lung tissue was ∼50°C.

Radiofrequency ablation using an internal cooled electrode with a power output of 30 W and flow rate of 40 mL·min−1. a) Power output (mean 23 W), b) temperature (mean 51°C) and c) impedance (increased from 245 to 189 Ω). d) Macroscopic findings showed a ring burn with central necrosis. e) Microscopic findings showed haemorrhage in the central area and diffuse alveolar destruction (haematoxylin-eosin stain; scale bar = 0.5 mm).
As shown in figure 5⇓, internal cooled-RFA was applied under the most appropriate conditions: 30 W power output and a flow rate of 40 mL·min−1 for 15, 30 and 60 s. The electrode tip temperature reached >50°C within 10 s at both water temperatures. The cooled-RFA with cold water achieved coagulation necrosis of ∼7 mm in diameter after 15 s of ablation. There was a major difference histologically between cold water and room temperature water. The macroscopic findings with room temperature water showed larger burn lesions than with cold water (40×45 and 20×15 mm, respectively) after 60 s of ablation; however, after 30 s of ablation, the burn size was almost identical between room temperature and cold water (11×7 mm and 7×5 mm, respectively). From these histological results, a 30-s exposure of RFA affected deeper lung tissues similarly, independent of the temperature of water used.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
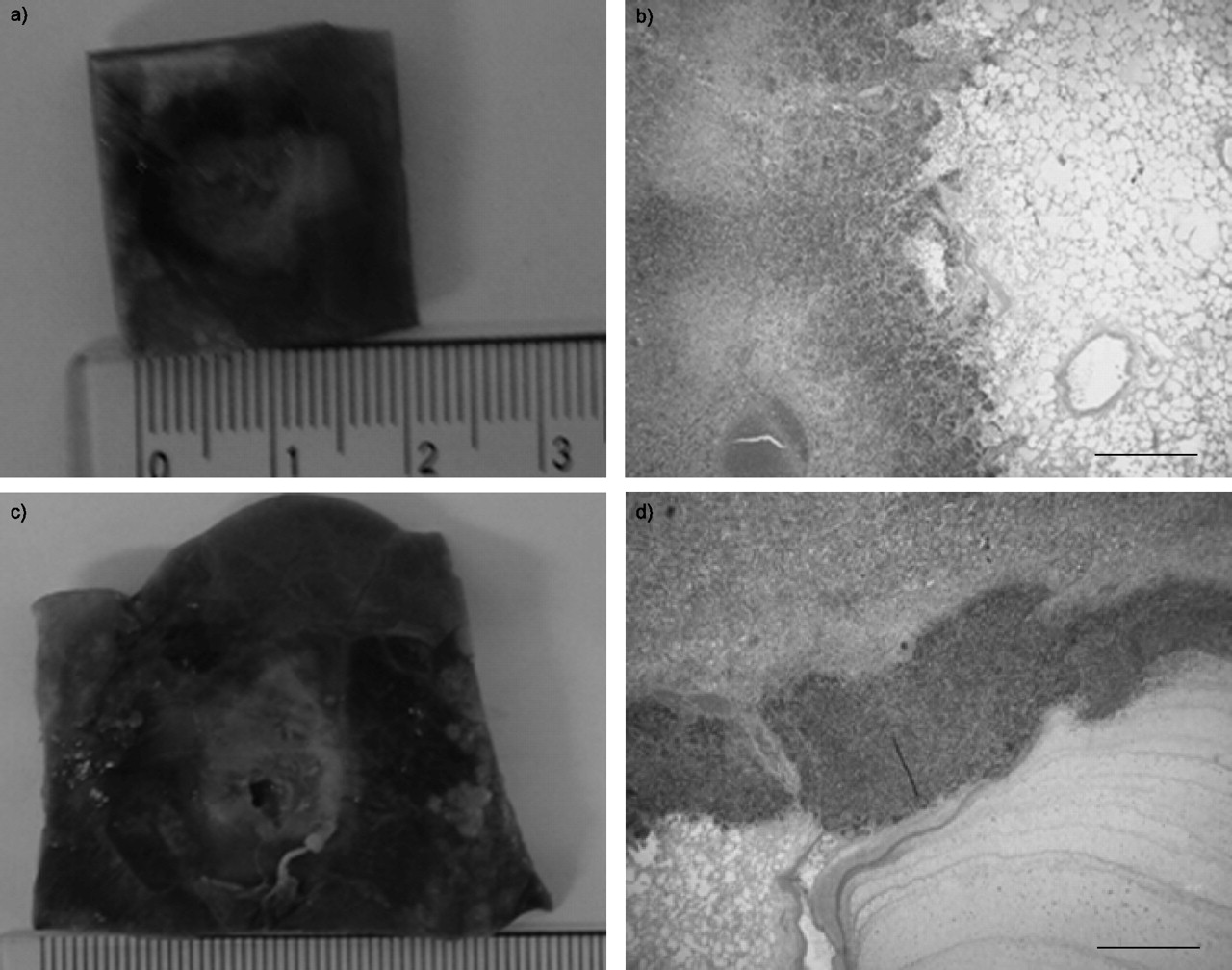
Radiofrequency ablation using an internal cooled electrode with a power output of 30 W, flow rate of 40 mL·min−1 and 60 s ablation time. a,b) Cold water (4°C) and c,d) room temperature water were used as an internal flow. Cold water showed coagulation necrosis of 15 mm in diameter and a burn area of 20 mm in diameter. c) Room temperature water showed coagulation necrosis of 15 mm in diameter and a burn area of ∼40 mm in diameter. The necrotic size was twice as large as that with cold water. b) and d) Microscopic findings indicate the border between the infiltration zone and normal lung; haemorrhage in the alveoli and diffuse alveolar destruction (haematoxylin-eosin stain; scale bar = 0.5 mm).
On ablation of the bronchial membrane, a sufficient necrotic effect was achieved with white denaturation of the mucous membrane within 10 s using a cooled-RFA with cold water. No bronchial perforation was observed within 30 s of ablation; however, since impedance increased faster compared with the peripheral lung tissue, RFA could not continue for >30 s. This was due to contact resistance around the electrode tip.
DISCUSSION
Percutaneous guided-RFA has found clinical applications for lung cancer with good results reported 4–7, 12. Since the electrode is placed percutaneously directly into the tumour, under cross-sectional imaging guidance such as chest CT, complications such as pneumothorax occur with frequency. The frequency of pneumothorax or haemothorax using a percutaneous method in a rabbit model was 47% 13 and clinical complications occur in 16–35% of percutaneously directly RFA 6, 7. However, it is possible to avoid these complications using the present fibreoptic bronchoscopy guidance; this is the greatest advantage of the authors’ internal cooled electrode. Fiberoptic bronchoscopy-guided cooled-RFA is both safe and technically feasible as the tip of the electrode is confirmed with CT or radiographic imaging guidance. As the present study has shown, cooled-RFA had no complications, such as bronchial bleeding or pneumothorax, and can be used with CT or radiographic imaging guidance technologies. Therefore, to the current authors’ knowledge, the present study is the first to demonstrate fibreoptic bronchoscopy-guided cooled-RFA as a potential therapeutic tool.
The peripheral lung is referred to as the safety zone; however, the anatomically central and middle bronchi are accompanied by the pulmonary artery branches. One complication anticipated with bronchoscopy is bronchial bleeding. The authors tried to ablate several areas of lesions from peripheral lung tissues to central lung tissues using power output of 30 W and flow rate of 40 mL·min−1 (data not shown). On day 7 after ablation there were no complications of macro bronchial haemorrhage from the middle or central artery or atelectasis. Therefore, the authors confirm that cooled-RFA achieved coagulation and haemostasis in the normal lung tissues although the safety in other lung tissues that may bleed more than normal lungs needs to be assessed.
This internal cooled-RFA is constructed as a thin catheter (diameter 1.67 mm) to pass through the bronchoscopy channel. The necrotic size obtained by this electrode is a critical consideration for this method. To achieve higher power output from the electrode and sufficient coagulation necrosis, it was necessary to increase the power output and to reduce impedance around the electrode tip. Using the standard noncooled electrode, the temperature around the tip rose rapidly and the pop phenomenon occurred in the lung tissues. This phenomenon means that coagulated necrotic tissue is formed around the electrode tip and tissue impedance increases rapidly. To avoid this phenomenon, the electrode tip should be cooled using water. On the basis of these results using a cooled-RFA for cardiac conduction disease 14, 15, it is predicted that the lesion occurs in lung tissues away from the cooled-RFA. The cooled-RFA enables greater power output for a longer time compared with the standard noncooled-RFA, resulting in larger coagulation necrosis area. The electrode tip is cooled by circulating water in the electrode catheter. As a result, the tissue temperature just around the electrode tip does not reach an excessive temperature. Based on this theory, the cooled-RFA can reach deeper and wider areas of ablation using the same power output. Therefore, as shown in the current results, the cooled-RFA could obtain coagulation necrosis compared with the standard noncooled-RFA, and the cooled-RFA using circulating room temperature water could obtain larger burn lesions than that using circulating cold water.
RFA is regarded as suitable for use on lung cancer as the radiofrequency energy to a tumour relies on the insulation effect by the existence of normal surrounding lungs 5. However, surgery is recognised as the standard treatment for patients with localised primary lung cancer and metastatic resectable lesions. A minimally invasive procedure such as RFA is usually considered in patients with a generally poor outcome following treatment with systemic chemotherapy and radiotherapy, patients with a poor cardiopulmonary status or coexistent medical problems for surgery. There have been some reports of RFA applied clinically for lung tumours 16, 17. The role of RFA in lung cancer is not sufficiently clear. However, bronchoscopy-guided RFA achieves only local coagulation necrosis and is likely to minimise injury to lung tissues and perhaps have a beneficial effect on a patient's condition. When institutions use RFA percutaneously, an epidural anaesthetic consisting of lidocaine, fentanyl or both as needed, needs to be administered percutaneously with an epidural tube 7. If this procedure could be applied to advanced human lung cancer, cooled-RFA could be used with the same method as usual biopsy forceps under topical lidocaine anaesthesia only. The advantages of bronchoscopy-guided cooled-RFA could include the ability to administer treatment nonsurgically as well as a shorter hospital stay for the patient. Based on the current results, it is suggested that RFA for advanced lung cancer might have numerous benefits over systemic chemotherapy or radiation therapy, although trials would be needed to confirm the potential risks/benefits.
One limitation of the present study is that potential tumours requiring ablation would most likely have a different behaviour, and data obtained on RFA in normal lungs cannot be extrapolated to tumour-bearing lungs. As VX2 tumour strains have strong malignant potential, some studies using RFA have been reported 13. As the current authors needed to perform bronchoscopy-guided RFA, larger animals such as sheep, dogs or pigs were required. The authors tried to inject VX2 tumour cells into the right or left lower lung of sheep, but the tumours cells did not grow in the lung. Secondly, as sheep skin is covered with wool, initial impedance was high compared with human lungs (initial impedance of humans: 130–200 Ω). Therefore, the size of coagulation necrosis may have been underestimated because the rapid increase of impedance could not achieve sufficiently long ablation time and power output. As shown in figure 5⇑, although the power output was set at 30 W, an average power output of 30 W was not achieved. However, since this method could achieve adequate coagulation necrosis, if it were applied in humans, larger coagulation necrosis would be achieved under the same conditions as the sheep lung with 30 W power output and a flow rate of 40 mL·min−1. As excessive coagulation necrosis on the surface of ablated sheep lung tissues was not achieved, RFA could be performed using circulating cold water in the electrode tip in humans.
In conclusion, internal bronchoscopy-guided cooled-radiofrequency ablation was a safe, effective and feasible procedure without major complications. The ideal power output of 30 W and a flow rate of 40 mL·min−1 were assessed as safe and technically feasible conditions for bronchoscopy-guided cooled-radiofrequency ablation for this normal sheep lung.
Acknowledgments
The authors would like to thank F. D'Alessio from Johns Hopkins University School of Medicine (Baltimore, MD, USA) for assistance with the language of the manuscript.
- Received August 26, 2006.
- Accepted February 21, 2007.
- © ERS Journals Ltd
References










